
Diabetes Mellitus
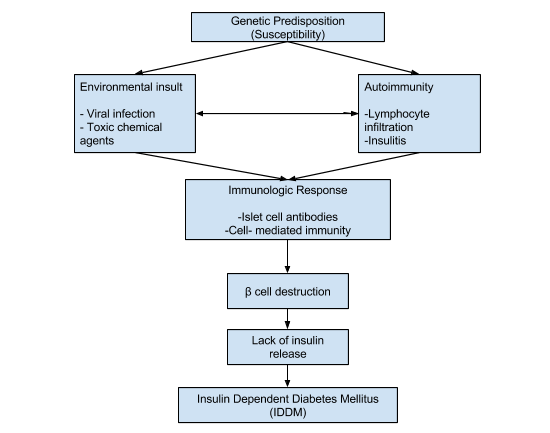
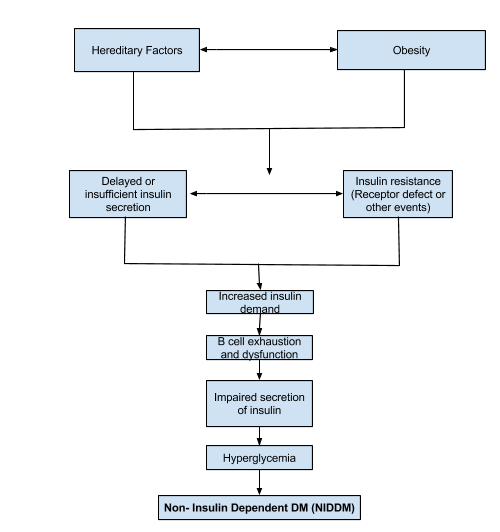
Diabetes, a chronic disease, is the result of the pancreas’ failure to produce sufficient amounts of insulin OR when the body cannot effectively use the insulin being produced. This leads to hyperglycemia, or high blood glucose concentration. There are 2 known types of diabetes. Type I is characterized by the lack of insulin production, while Type II is characterized by ineffective use of insulin, often as a result of excess body weight and physical inactivity. There is also gestational diabetes, which is seen in pregnancy.
Nursing Diagnoses
Risk for infection
Risk factors may include
- High glucose levels
- Decreased leukocyte function
- Alterations in circulation
- Pre-existing respiratory infection
- Urinary tract infection
Desired outcomes
- Identify interventions to reduce the risk of infection
- Demonstrate techniques, lifestyle changes to prevent development of infection
Nursing interventions
| INTERVENTION | RATIONALE |
| Observe for the signs of infection and inflammation: fever, flushed appearance, wound drainage, purulent sputum, cloudy urine. | Patients with DM may be admitted with infection, which could have precipitated the ketoacidotic state. They may also develop nosocomial infection. |
| Teach and promote good hand hygiene. | Reduces risk of cross-contamination. |
| Maintain asepsis during IV insertion, administration of medications, and providing wound or site care. Rotate IV sites as indicated. | Increased glucose in the blood creates an excellent medium for bacteria to thrive. |
| Provide catheter or perineal care. Teach female patients to clean from front to back after elimination. | Minimizes risk of UTI. Comatose patients may be at particular risk if urinary retention occurred before hospitalization. Note: Elderly female diabetic patients are especially prone to urinary tract and/or vaginal yeast infections. |
| Provide meticulous skin care: gently massage bony areas, keep skin dry. Keep linens dry and wrinkle-free. | Peripheral circulation may be ineffective or impaired, placing the patient at increased risk for skin breakdown and infection. |
| Auscultate breath sounds. | Rhonchi may indicate accumulation of secretions possibly related to pneumonia or bronchitis. Crackles may result from pulmonary congestion or edema from rapid fluid replacement or heart failure. |
| Place in semi-Fowler’s position. | Facilitates lung expansion; reduces risk of aspiration |
| Reposition and encourage coughing or deep breathing if the patient is alert and cooperative. Otherwise, suction airway using sterile technique as needed. | Aids in ventilating all lung areas and mobilizing secretions. Prevents stasis of secretions with increased risk of infection. |
| Provide tissues and trash bags in a convenient location for sputum and other secretions. Instruct patients in proper handling of secretions. | To minimize the spread of infection. |
| Encourage and assist with oral hygiene. | Reduces risk of oral/gum disease. |
| Encourage adequate dietary and fluid intake (approximately 3000 mL/day if not contraindicated by cardiac or renal dysfunction), including 8 oz of cranberry juice per day as appropriate. | Decreases susceptibility to infection. Increased urinary flow prevents stasis and aids in maintaining urine pH/acidity, reducing bacteria growth and flushing organisms out of the system. Note: Use of cranberry juice can help prevent bacteria from adhering to the bladder wall, reducing the risk of recurrent UTI. |
| Administer antibiotics as appropriate. | Early treatment may help prevent sepsis. |
Risk for disturbed sensory perception
Risk factors may include
- Endogenous chemical alteration
- Glucose/insulin imbalance
- Electrolyte imbalance
Desired outcomes
- Maintain usual level of mentation
- Recognize and compensate for existing sensory impairments
Nursing interventions
| Monitor vital signs and mental status. | To provide a baseline from which to compare abnormal findings. |
| Call the patient by name, reorient as needed to place, person, and time. Give short explanations, speak slowly and enunciate clearly. | Decreases confusion and helps maintain contact with reality. |
| Schedule and cluster nursing time and interventions. | To provide uninterrupted rest periods and promote restful sleep, minimize fatigue and improve cognition. |
| Keep the patient’s routine as consistent as possible. Encourage participation in activities of daily living (ADLs) as able. | Helps keep patient in touch with reality and maintain orientation to the environment. |
| Protect patients from injury by avoiding or limiting the use of restraints as necessary when LOC is impaired. Place the bed in a low position and pad bed rails if the patient is prone to seizures. | Disoriented patients are prone to injury, especially at night, and precautions need to be taken as indicated. Seizure precautions need to be taken as appropriate to prevent physical injury, aspiration, and falls. |
| Evaluate visual acuity as indicated. | Retinal edema or detachment, hemorrhage, presence of cataracts or temporary paralysis of extraocular muscles may impair vision, requiring corrective therapy and/or supportive care. |
| Observe and investigate reports of hyperesthesia, pain, or sensory loss in the feet or legs. Investigate and look for ulcers, reddened areas, pressure points, loss of pedal pulses. | Peripheral neuropathies may result in severe discomfort, lack of or distortion of tactile sensation, potentiating risk of dermal injury and impaired balance. |
| Provide bed cradle. Keep hands and feet warm, avoiding exposure to cool drafts and/or hot water or use of heating pad. | Reduces discomfort and potential for dermal injury. Assist patient with ambulation or position changes. |
| Assist patient with ambulation or position changes. | Promotes patient safety, especially when sense of balance is affected. |
| Monitor laboratory values: blood glucose, serum osmolality, Hb/Hct, BUN/Cr. | Imbalances can impair mentation. Note: If fluid is replaced too quickly, excess water may enter brain cells and cause alteration in the level of consciousness (water intoxication). |
| Carry out prescribed regimen for correcting DKA as indicated. | Alteration in thought processes or potential for seizure activity is usually alleviated once hyperosmolar state is corrected. |
Powerlessness
- Long-term/progressive illness that is not curable
- Dependence on others
Possibly evidenced by
- Reluctance to express true feelings; expressions of having no control/influence over situation
- Apathy, withdrawal, anger
- Does not monitor progress, nonparticipation in care/decision making
- Depression over physical deterioration/complications despite patient cooperation with regimen
Desired outcomes
- Acknowledge feelings of helplessness
- Identify healthy ways to deal with feelings
- Assist in planning own care and independently take responsibility for self-care activities
Nursing interventions
| INTERVENTION | RATIONALE |
| Discuss with patient the need for activity. Plan schedule with patient and identify activities that lead to fatigue. | Education may provide motivation to increase activity level even though patient may feel too weak initially. |
| Alternate activity with periods of rest and uninterrupted sleep. | To prevent excessive fatigue. |
| Monitor pulse, respiratory rate, and BP before and after activity. | Indicates physiological levels of tolerance. |
| Discuss ways of conserving energy while bathing, transferring, and so on. | Patient will be able to accomplish more with a decreased expenditure of energy. |
| Increase patient participation in ADLs as tolerated. | Increases confidence level, self-esteem and tolerance level. |
Possibly evidenced by
- Elevated temperature
- Increased urine output
- Sweating
- Thirst
- Exhaustion
- Weight loss
- Dry skin and/or mucous membrane
Desired outcomes
- Patient will verbalize understanding of causative factors and purpose of individual therapeutic interventions and medications.
- Patient will improve or maintain fluid volume at a functional level as evidenced by individual good skin turgor, moist mucous membrane, and stable vital signs.
Nursing interventions
| INTERVENTION | RATIONALE |
| Establish rapport. | Friendly and trusting relationship with patient and to be able to understand each other’s concern. |
| Take and record vital signs. | To obtain baseline data. |
| Monitor the temperature. | To monitor changes in temperature. |
| Assess skin turgor and mucous membranes for signs of dehydration. | Dry mucous membranes are signs of dehydration. |
| Monitor intake and output. | To assess for signs of dehydration. |
| Encourage patient to increase fluid intake as tolerated. | To replace fluid loss and prevent dehydration. |
| Administer IVF as ordered. | To replace lost electrolytes and fluids. |
Imbalanced Nutrition: less than body requirement r/t insulin deficiency
Possibly evidenced by
- Poor muscle tone
- Generalized weakness
- Increased thirst
- Increased urination
- Polyphagia
- Loss of weight
Desired outcomes
- Patient will verbalize understanding of causative factors when known and necessary interventions are identified for diabetic client.
- Patient will demonstrate improvement of weight and nutrition towards goal.
Nursing interventions
| INTERVENTION | RATIONALE |
| Ascertain understanding of individual nutritional needs. | To determine what information to be provided to client or SO. |
| Discuss eating habits and encourage diabetic diet (balanced diet) as prescribed by the doctor. | To achieve health needs of the patient with the proper food diet for his condition. |
| Document actual weight, do not estimate. Note total daily intake including patterns and time of eating. | Patients may be unaware of their actual weight or weight loss due to estimation of weight. |
| Consult dietician and/or physician for further assessment and recommendation regarding food preferences and nutritional support. | To reveal changes that should be made in the client’s dietary intake. For greater understanding and further assessment of specific foods. |
Risk for infection
Risk factors
- Chronic hyperglycemia
- Neurogenic bladder
- Peripheral vascular disease
Desired outcomes
- Patient will be free of infections as evidenced by normothermia, negative cultures, and WBC within normal levels.
Nursing interventions
| INTERVENTION | RATIONALE |
| Assess temperature every four (4) hours. Notify physician if fever occurs. | Fever is a sign of an infection Infection is the most common cause of diabetic ketoacidosis (DKA). |
| Monitor for signs of infection (e.g., fever, rhonchi, dyspnea, and/or cough). | These are indicators of pneumonia which is common among patients with DM. |
| Assess for dysuria, tachycardia, diaphoresis, nausea, vomiting, and abdominal pain. | These are indicators of UTI. Neurogenic bladder predisposes to UTI. |
| Assess for erythema, swelling, and purulent drainage at IV sites. | These are signs of IV catheter infections. |
Risk of Impaired Skin Integrity
Risk factors
- Decreased circulation and sensation caused by peripheral neuropathy and arterial obstruction.
Desired outcomes
- Patient’s skin on legs and feet remains intact while the patient is hospitalized.
- Patient will demonstrate proper foot care.
Nursing interventions
| INTERVENTION | RATIONALE |
| Assess integrity of the skin. Assess knee and deep tendon reflexes and proprioception. | These are assessments for neuropathy. Skin on lower extremity pressure points is at great risk for ulceration. |
| Use foot cradle on the bed. Use space boots on ulcerated heels, elbow protectors, and pressure-relief mattresses. | To prevent pressure on pressure-sensitive points. |
| Wash feet daily with mild soap and warm water. Check water temperature before immersing feet in the water. | Decreased sensation increases the risk for burns. |
| Inspect feet daily for erythema or trauma. | These are signs that the skin needs preventive care. |
| Change socks or stockings daily. Encourage the patient to wear white cotton socks. | To prevent infection from moisture. White fabric enables easy visualization of blood or exudates. |
| Use gentle moisturizers on the feet. | Moisturizers soften and lubricate dry skin, preventing skin cracking. |
| Cut toenails straight across after softening toenails with a bath. | This action prevents ingrown toenails, which could cause infection. |
| The patient should not walk barefoot. | This is a high risk for trauma and may result in ulceration and infection. |
Nursing Notes
Type I vs. Type II Diabetes
| PE I (IDDM)1 | TYPE II (NIDDM) | |
| Description | Partly inherited and triggered by certain infections; requires an environmental trigger | Due primarily to lifestyle factors and genetics |
| Age of onset | Typically <40 years old | Typically >40 years old |
| Body weight | Thin | Typically overweight |
| Symptoms | Sudden onset | Insidious onset |
| Insulin produced | None | Too little, or ineffective |
| Insulin requirements | Exogenous insulin required | May require insulin |
Signs & Symptoms
The classic symptoms of untreated diabetes are loss of weight, polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger). Symptoms may develop rapidly (weeks or months) in type 1 diabetes, while they usually develop much more slowly and may be subtle or absent in type 2 diabetes.
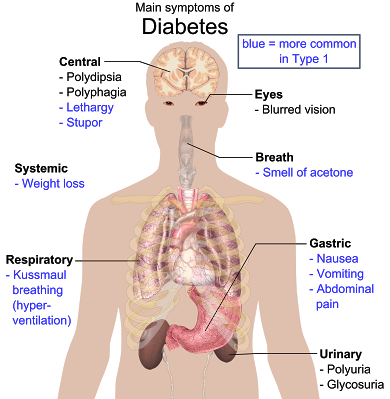
Prolonged high blood glucose can cause glucose absorption in the lens of the eye, which leads to changes in its shape, resulting in vision changes. Blurred vision is a common complaint leading to a diabetes diagnosis; type 1 should always be suspected in cases of rapid vision change, whereas with type 2 change is generally more gradual, but should still be suspected.
A number of skin rashes that can occur in diabetes are collectively known as diabetic dermadromes.
Diagnostic Procedure
- Random blood glucose test
- Blood can be drawn at any time of the day (regardless of patient’s last meal)
- > 200 mg/dL (11.1 mmol/L) in persons with high blood glucose symptoms suggests a diabetes diagnosis
- Fasting blood glucose test
- Measure blood after not eating or drinking for 8 to 12 hours (typically overnight)
- Normal blood glucose: <100 mg/dL
- Diabetic: > 126 mg/dL (7.0 mmol/L)
- Take a small sample of blood from vein or fingertip; repeat on another day
- Hemoglobin A1C test
- Measures average blood glucose level during the past 2-3 months
- Used to monitor blood glucose control in people with known diabetes
- Not normally used to diagnose diabetes
- Normal: 4-6%
- Oral glucose test
- Most sensitive test for diagnosing diabetes & pre-diabetes
- Not routinely recommended; inconvenient
- Includes a fasting blood glucose