Liver Cirrhosis
Liver cirrhosis is a chronic disease where hepatic tissue cells are destroyed and eventually fibrose. Laennec’s (Alcohol-Induced) Cirrhosis, the most common form, results from chronic alcoholism and malnutrition, with fibrosis occuring in the central and portal areas. Postnecrotic (Micronodular) Cirrhosis results from previous acute viral hepatitis and/or drug-induced massive hepatic necrosis, giving rise to scar tissue. The third form is Biliary Cirrhosis which is caused by chronic biliary obstruction and infection, leading to scarred bile ducts and liver lobes. In effect, the normal liver structure and vasculature are affected, blood and lymph flow are impaired, resulting in hepatic insufficiency and portal vein hypertension. If left untreated, it can lead to hyponatremia, water retention, bleeding esophageal varices, coagulopathy, bacterial peritonitis, and hepatic encephalopathy.
Nursing Diagnoses
Undernutrition
May be related to
- Inadequate diet; inability to process/digest nutrients
- Anorexia, nausea/vomiting, indigestion, early satiety (ascites)
- Abnormal bowel function
Possibly evidenced by
- Weight loss
- Changes in bowel sounds and function
- Poor muscle tone/wasting
- Imbalances in nutritional studies
Desired outcomes
- Demonstrate progressive weight gain toward goal with patient-appropriate normalization of laboratory values
- Experience no further signs of malnutrition
Nursing interventions
| INTERVENTION | RATIONALE |
| Measure dietary intake by calorie count | Provides important information about intake, needs and deficiencies |
| Weigh as indicated. Compare changes in fluid status, recent weight history, skinfold measurements | It may be difficult to use weight as a direct indicator of nutritional status in view of edema and/or ascites. Skinfold measurements are useful in assessing changes in muscle mass and subcutaneous fat reserves. |
| Encourage patients to eat; explain reasons for the types of diet. Feed patients if tiring easily, or have SO assist patients. Include the patient in meal planning to consider his/her preferences in food choices. | Improved nutrition and diet is vital to recovery. Patients may eat better if family is involved and preferred foods are included as much as possible. |
| Encourage patients to eat all meals including supplementary feedings. | Patients may pick at food or eat only a few bites because of loss of interest in food or because of nausea, generalized weakness, or malaise. |
| Give small, frequent meals. | Poor tolerance to larger meals may be due to increased intra-abdominal pressure and ascites (if present). |
| Provide salt substitutes, if allowed; avoid those containing ammonium. | Salt substitutes enhance the flavor of food and aid in increasing appetite; ammonia potentiates risk of encephalopathy. |
| Restrict intake of caffeine, gas-producing or spicy and excessively hot or cold foods. | Aids in reducing gastric irritation and/or diarrhea and abdominal discomfort that may impair oral intake. |
| Suggest soft foods, avoiding roughage if indicated. | Hemorrhage from esophageal varices may occur in advanced cirrhosis. |
| Encourage frequent mouth care, especially before meals. | Patient is prone to sore and/or bleeding gums and bad taste in the mouth, which contributes to anorexia. |
| Promote undisturbed rest periods, especially before meals. | Conserving energy reduces metabolic demands on the liver and promotes cellular regeneration. |
| Recommend cessation of smoking. Provide teaching on the possible negative effects of smoking. | Reduces excessive gastric stimulation and risk of irritation and may lead to bleeding. |
| Monitor laboratory studies: serum glucose, prealbumin and albumin, total protein, ammonia. | Glucose may be decreased because of impaired gluconeogenesis, depleted glycogen stores, or inadequate intake. Protein may be low because of impaired metabolism, decreased hepatic synthesis, or loss into peritoneal cavity (ascites). Elevation of ammonia level may require restriction of protein intake to prevent serious complications. |
| Maintain NPO status when indicated | Initially, GI rest may be required in acutely ill patients to reduce demands on the liver and production of ammonia and urea in the GI tract. |
| Refer to a dietitian to provide a diet high in calories and simple carbohydrates, low in fat, and moderate to high in protein; limit sodium and fluid as necessary. Provide liquid supplements as indicated. | High-calorie foods are desired inasmuch as patient intake is usually limited. Carbohydrates supply readily available energy. Fats are poorly absorbed because of liver dysfunction and may contribute to abdominal discomfort. Proteins are needed to improve serum protein levels to reduce edema and to promote liver cell regeneration. Note: Protein and foods high in ammonia (gelatin) are restricted if ammonia level is elevated or if a patient has clinical signs of hepatic encephalopathy. In addition, these individuals may tolerate vegetable protein better than meat protein. |
| Provide tube feedings, TPN, lipids if indicated. | May be required to supplement diet or to provide nutrients when a patient is too nauseated or anorexic to eat or when esophageal varices interfere with oral intake. |
Fluid Volume Excess
May be related to
- Compromised regulatory mechanism (e.g., syndrome of inappropriate antidiuretic hormone [SIADH], decreased plasma proteins, malnutrition)
- Excess sodium/fluid intake
Possibly evidenced by
- Edema, anasarca, weight gain
- Intake greater than output, oliguria, changes in urine specific gravity
- Dyspnea, adventitious breath sounds, pleural effusion
- BP changes, altered CVP
- JVD, positive hepatojugular reflex
- Altered electrolyte levels
- Change in mental status
Desired outcomes
- Demonstrate stabilized fluid volume, with balanced I&O, stable weight, vital signs within patient’s normal range, and absence of edema.
Nursing interventions
| INTERVENTION | RATIONALE |
| Measure I&O, weigh daily, and note gain of more than 0.5 kg/day. | To assess circulating volume status, developing or resolution of fluid shifts, and response to therapeutic regimen. Positive balance/weight gain often reflects continuing fluid retention. Note: Decreased circulating volume (fluid shifts) may directly affect renal function and urine output, resulting in hepatorenal syndrome. |
| Monitor BP (and CVP if available). Note JVD and abdominal vein distension. | BP elevations are usually associated with fluid volume excess but may not occur because of fluid shifts out of the vascular space. Distension of external jugular and abdominal veins is associated with vascular congestion. |
| Assess respiratory status, noting increased respiratory rate, dyspnea. | Indicative of pulmonary congestion. |
| Auscultate lungs, noting diminished breath sounds and developing adventitious sounds. | Increasing pulmonary congestion may result in consolidation, impaired gas exchange, and complications. |
| Monitor for cardiac dysrhythmias. Auscultate heart sounds, noting development of S3/S4 gallop rhythm. | May be caused by HF, decreased coronary arterial perfusion, and electrolyte imbalance. |
| Assess degree of peripheral edema. | Fluids shift into tissues as a result of sodium and water retention, decreased albumin, and increased antidiuretic hormone (ADH). |
| Measure abdominal girth. | Reflects accumulation of fluid (ascites) resulting from loss of plasma proteins/fluid into peritoneal space. Note: Excessive fluid accumulation can reduce circulating volume, creating a deficit (signs of dehydration). |
| Encourage bedrest when ascites is present. | May promote recumbency induced diuresis. |
| Provide frequent mouth care; occasional ice chips (if NPO). | Decreases sensation of thirst. |
| Monitor serum albumin and electrolytes (particularly potassium and sodium). | Decreased serum albumin affects plasma colloid osmotic pressure, resulting in edema formation. Reduced renal blood flow accompanied by elevated ADH and aldosterone levels and the use of diuretics (to reduce total body water) may cause various electrolyte shifts/imbalances. |
| Monitor serial chest x-rays. | Vascular congestion, pulmonary edema, and pleural effusions frequently occur. |
| Restrict sodium and fluids as indicated. | Sodium may be restricted to minimize fluid retention in extravascular spaces. Fluid restriction may be necessary to correct dilutional hyponatremia. |
| Administer salt-free albumin/plasma expanders as indicated. | Albumin may be used to increase the colloid osmotic pressure in the vascular compartment (pulling fluid into vascular space), thereby increasing effective circulating volume and decreasing formation of ascites. |
Administering analgesics
| INTERVENTION | RATIONALE |
| Diuretics: spironolactone (Aldactone), furosemide (Lasix) | Used with caution to control edema and ascites, block the effect of aldosterone, and increase water excretion while sparing potassium when conservative therapy with bedrest and sodium restriction does not alleviate the problem. |
| Potassium | Serum and cellular potassium are usually depleted because of liver disease and urinary losses. |
| Positive inotropic drugs and arterial vasodilators | Given to increase cardiac output/improve renal blood flow and function, thereby reducing excess fluid. |
Risk for Impaired Skin Integrity
Risk factors may include
- Altered circulation/metabolic state
- Accumulation of bile salts in skin
- Poor skin turgor, skeletal prominence, presence of edema, ascites
Desired outcomes
- Maintain skin integrity
- Identify individual risk factors and demonstrate behaviors/techniques to prevent skin breakdown
Nursing interventions
| INTERVENTION | RATIONALE |
| Inspect pressure points and skin surfaces closely and routinely. Gently massage bony prominences or areas of continued stress. Use of emollient lotions and limiting use of soap for bathing may help. | Edematous tissues are more prone to breakdown and to the formation of decubitus. Ascites may stretch the skin to the point of tearing in severe cirrhosis. |
| Encourage and assist patients with reposition on a regular schedule. Assist with active and passive ROM exercises as appropriate. | Repositioning reduces pressure on edematous tissues to improve circulation. Exercises enhance circulation and improve and/or maintain joint mobility. |
| Recommend elevating lower extremities. | Enhances venous return and reduces edema formation in extremities. |
| Keep linens dry and free of wrinkles. | Moisture aggravates pruritus and increases risk of skin breakdown. |
| Suggest clipping fingernails short; provide mittens/gloves if indicated. | Prevents patients from inadvertently injuring the skin, especially while sleeping. |
| Provide perineal care following urination and bowel movement. | Prevents skin excoriation breakdown from bile salts. |
| Use an alternating pressure mattress, egg-crate mattress, waterbed, sheepskins, as indicated. | Reduces dermal pressure, increases circulation, and diminishes risk of tissue ischemia. |
| Use calamine lotion and provide baking soda baths. Administer medications (as indicated) such as cholestyramine (Questran), hydroxyzine (Atarax), diphenhydramine (Benadryl). | May be soothing and can provide relief of itching associated with jaundice, bile salts in skin. |
Risk for Ineffective Breathing Pattern
Risk factors may include
- Intra-abdominal fluid collection (ascites)
- Decreased lung expansion, accumulated secretions
- Decreased energy, fatigue
Desired outcomes
- Maintain effective respiratory pattern; be free of dyspnea and cyanosis, with ABGs and vital capacity within acceptable range
Nursing interventions
| INTERVENTION | RATIONALE |
| Monitor respiratory rate, depth, and effort. | Rapid shallow respiration or presence of dyspnea may appear because of hypoxia and/or fluid accumulation in the abdomen. |
| Auscultate breath sounds, noting crackles, wheezes, rhonchi. | May indicate developing complications. Presence of adventitious breath sounds may reflect accumulation of fluids or secretions. Absent or diminished sounds suggest atelectasis. |
| Investigate changes in level of consciousness. | Changes in mentation may reflect hypoxemia and respiratory failure, which often accompany hepatic coma. |
| Keep the head of the bed elevated. Position on sides. | Facilitates breathing by reducing pressure on the diaphragm, and minimizes risk of aspiration of secretions. |
| Encourage frequent repositioning and deep-breathing exercises and coughing exercises. | Aids in lung expansion and mobilizing secretions. |
| Monitor temperature. Note presence of chills, increased coughing, changes in color and character of sputum. | Indicative of onset of infection, especially pneumonia. |
| Monitor serial ABGs, pulse oximetry, vital capacity measurements, chest x-rays. | Reveals changes in respiratory status, developing pulmonary complications. |
| Provide supplemental O2 as indicated. | To treat or prevent hypoxia and if respirations and oxygenation is inadequate, mechanical ventilation may be required. |
| Demonstrate and assist with respiratory adjuncts: incentive spirometer. | Reduces incidence of atelectasis, enhances mobilization of secretions. |
Risk for Injury (Hemorrhage)
Risk factors may include
- Abnormal blood profile; altered clotting factors (decreased production of prothrombin, fibrinogen, and factors VIII, IX, and X; impaired vitamin K absorption; and release of thromboplastin)
- Portal hypertension, development of esophageal varices
Desired outcomes
- Maintain homeostasis with absence of bleeding
- Demonstrate behaviors to reduce risk of bleeding.
Nursing interventions
| INTERVENTION | RATIONALE |
| Closely assess for signs and symptoms of GI bleeding: check all secretions for frank or occult blood. Observe color and consistency of stools, NG drainage, or vomitus | The esophagus and rectum are the most usual sources of bleeding because of their mucosal fragility and alterations in hemostasis associated with cirrhosis. |
| Observe the presence of petechiae, ecchymosis, bleeding from one or more sites. | Subacute disseminated intravascular coagulation (DIC) may develop secondary to altered clotting factors. |
| Monitor pulse, BP (and CVP if available). | An increased pulse with decreased BP and CVP can indicate loss of circulating blood volume, requiring further evaluation. |
| Note changes in mentation and LOC. | Changes may indicate decreased cerebral perfusion secondary to hypovolemia, hypoxemia. |
| Avoid rectal temperature; be gentle with GI tube insertions. | Rectal and esophageal vessels are most vulnerable to rupture. |
| Encourage use of soft toothbrush, electric razor, avoiding straining for stool, vigorous nose blowing, and so forth. | In the presence of clotting factor disturbances, minimal trauma can cause mucosal bleeding. |
| Use small needles for injections. Apply pressure to small bleeding and venipuncture sites for longer than usual. | Minimizes damage to tissues, reducing risk of bleeding and hematoma. |
| Advice to avoid aspirin-containing products. | Prolongs coagulation, potentiating risk of hemorrhage. |
| Monitor Hb/Hct and clotting factors. | Indicators of anemia, active bleeding, or impending complications. |
Administering medications
| INTERVENTION | RATIONALE |
| Supplemental vitamins: vitamin K, D, and C. | Promotes prothrombin synthesis and coagulation if the liver is functional. Vitamin C deficiencies increase susceptibility of the GI system to irritation and/or bleeding. |
| Stool softeners | Prevents straining for stool with resultant increase in intra-abdominal pressure and risk of vascular rupture and hemorrhage. |
| Provide gastric lavage with room temperature and cool saline solution or water as indicated. | In the presence of acute bleeding, evacuation of blood from GI tract reduces ammonia production and risk of hepatic encephalopathy. |
| Assist with insertion and maintenance of GI tube. | Temporarily controls bleeding of esophageal varices when controlled by other means (e.g., lavage) and hemodynamic stability cannot be achieved. |
| Prepare for surgical procedures: direct ligation (banding) or varices, esophagogastric resection, splenorenal-portacaval anastomosis. | May be needed to control active hemorrhage or to decrease portal and collateral blood vessel pressure to minimize risk of recurrence of bleeding. |
Risk for Acute Confusion
Risk factors may include
- Alcohol abuse
- Inability of liver to detoxify certain enzymes/drugs
Desired outcomes
- Maintain usual level of mentation/reality orientation
- Initiate behaviors/lifestyle changes to prevent or minimize recurrence of problem
Nursing interventions
| INTERVENTION | RATIONALE |
| Observe signs and symptoms of behavioral change and mentation: lethargy, confusion, drowsiness, slurring of speech, and irritability. Around patients at intervals as indicated. | Ongoing assessment of behavior and mental status is important because of the fluctuating nature of impending hepatic coma. |
| Review current medication regimen. Note adverse drug reactions and effects of medication to the patient. | Adverse drug reactions or interactions (e.g., cimetidine plus antacids) may potentiate and/or exacerbate confusion. |
| Evaluate sleep and rest schedule. | Difficulty falling or staying asleep leads to sleep deprivation, resulting in diminished cognition and lethargy. |
| Note development and/or presence of asterixis, fetor hepaticus, seizure activity. | Suggests elevating serum ammonia levels; increased risk of progression to encephalopathy. |
| Consult with SO about the patient’s usual behavior and mentation. | Provides a baseline for comparison of current status. |
| Have patients write names periodically and keep this record for comparison. Report deterioration of ability. Have patients do simple arithmetic computations. | Easy test of neurological status and muscle coordination. |
| Reorient to time, place, person as needed. | Assists in maintaining reality orientation, reducing confusion and anxiety. |
| Maintain a pleasant, quiet environment and approach in a slow, calm manner. Encourage uninterrupted rest periods. | Reduces excessive stimulation and sensory overload, promotes relaxation, and may enhance coping. |
| Provide continuity of care. If possible, assign the same nurse over a period of time. | Familiarity provides reassurance, aids in reducing anxiety, and provides a more accurate documentation of subtle changes. |
| Reduce provocative stimuli, confrontation. Refrain from forcing activities. Assess potential for violent behavior. | Avoids triggering agitated, violent responses; promotes patient safety. |
| Discuss current situation, future expectation. | Patient/SO may be reassured that intellectual (as well as emotional) function may improve as liver involvement resolves. |
| Maintain bedrest, assist with self-care activities. | Reduces metabolic demands on liver, prevents fatigue, and promotes healing, lowering risk of ammonia buildup. |
| Identify and provide safety needs. Supervise during smoking, put the bed in low position, raise side rails and pad if necessary. | Reduces risk of injury when confusion, seizures, or violent behavior occurs. |
| Investigate temperature elevations. Monitor for signs of infection. | Infection may precipitate hepatic encephalopathy caused by tissue catabolism and release of nitrogen. |
| Recommend avoidance of narcotics or sedatives, anti anxiety agents, and limiting or restricting use of medications metabolized by the liver. | Certain drugs are toxic to the liver, whereas other drugs may not be metabolized because of cirrhosis, causing cumulative effects that affect mentation, mask signs of developing encephalopathy, or precipitate coma. |
| Eliminate or restrict protein in diet. Provide glucose supplements, adequate hydration. | Ammonia (product of the breakdown of protein in the GI tract) is responsible for mental changes in hepatic encephalopathy. Dietary changes may result in constipation, which also increases bacterial action and formation of ammonia. Glucose provides a source of energy, reducing need for protein catabolism. Note: Vegetable protein may be better tolerated than meat protein. |
| Assist with procedures as indicated: dialysis, plasmapheresis, or extracorporeal liver perfusion. | May be used to reduce serum ammonia levels if encephalopathy develops and other measures are not successful. |
Disturbed Body Image/Self-Esteem
May be related to
- Biophysical changes/altered physical appearance
- Uncertainty of prognosis, changes in role function
- Personal vulnerability
- Self-destructive behavior (alcohol-induced disease)
Possible evidenced by
- Verbalization of change/restriction in lifestyle
- Fear of rejection or reaction by others
- Negative feelings about body/abilities
- Feelings of helplessness, hopelessness, or powerlessness
Desired outcomes
- Verbalize understanding of changes and acceptance of self in the present situation.
- Identify feelings and methods for coping with negative perception of self.
Nursing interventions
| INTERVENTION | RATIONALE |
| Discuss situations and encourage verbalization of fears and concerns. Explain the relationship between the nature of disease and symptoms. | Patients are very sensitive to body changes and may also experience feelings of guilt when cause is related to alcohol or other drug use. |
| Support and encourage patients; provide care with a positive, friendly attitude. | Caregivers sometimes allow judgmental feelings to affect the care of patients and need to make every effort to help patients feel valued as a person. |
| Encourage family/SO to verbalize feelings, visit freely and participate in care. | Family members may feel guilty about a patient’s condition and may be fearful of impending death. They need nonjudgmental emotional support and free access to patients. Participation in care helps them feel useful and promotes trust between staff, patient, and SO. |
| Assist patient/SO to cope with change in appearance; suggest clothing that does not emphasize altered appearance (color of clothes, etc). | Patients may present an unattractive appearance as a result of jaundice, ascites, and ecchymotic areas. Providing support can enhance self-esteem and promote patient sense of control. |
| Refer to support services. Counselors, psychiatric resources, social service, clery and alcohol treatment programs may help. | Increased vulnerability and concerns associated with this illness may require services of additional professional resources. |
Deficient Knowledge
May be related to
- Lack of exposure/recall; information misinterpretation
- Unfamiliarity with information resources
Possible evidenced by
- Questions; request for information, statement of misconception
- Inaccurate follow-through of instructions/development of preventable complications
Desired outcomes
- Verbalize understanding of disease process/prognosis, potential complications.
- Correlate symptoms with causative factors.
- Identify/initiate necessary lifestyle changes and participate in care.
Nursing interventions
| INTERVENTION | RATIONALE |
| Review disease process and prognosis and future expectations. | Provides a knowledge base from which patients can make informed choices. |
| Refer to a dietitian or nutritionist. | Patients with cirrhosis need close observation and sound nutritional counseling. |
| Stress importance of avoiding alcohol. Give information about community services available to aid in alcohol rehabilitation if indicated. | Alcohol is the leading cause in the development of cirrhosis. |
| Inform patients of altered effects of medications with cirrhosis and the importance of using only drugs prescribed or cleared by a healthcare provider who is familiar with the patient’s history. | Some drugs are hepatotoxic (especially narcotics, sedatives, and hypnotics). In addition, the damaged liver has a decreased ability to metabolize all drugs, potentiating cumulative effect and/or aggravation of bleeding tendencies. |
| Review procedure for maintaining function of peritoneovenous shunt when present. | Insertion of a Denver shunt requires the patient to periodically pump the chamber to maintain patency of the device. Patients with a LeVeen shunt may wear an abdominal binder and/or engage in a Valsalva maneuver to maintain shunt function. |
| Assist patient identifying support person(s). | Because of length of recovery, potential for relapses, and slow convalescence, support systems are extremely important in maintaining behavior modifications. |
| Emphasize the importance of good nutrition. Recommend avoidance of high-protein/salty foods, onions, and strong cheeses. Provide written dietary instructions. | Proper dietary maintenance and avoidance of foods high in sodium and protein aid in remission of symptoms and help prevent ammonia buildup and further liver damage. Written instructions are helpful for patient to refer to at home. |
| Stress necessity of follow-up care and adherence to therapeutic regimen. | Chronic nature of disease has the potential for life-threatening complications. Provides opportunity for evaluation of effectiveness of regimen, including patency of shunt if used. |
| Discuss sodium and salt substitute restrictions and necessity of reading labels on food and OTC drugs. | Minimizes ascites and edema formation. Overuse of substitutes may result in other electrolyte imbalances. Food, OTC and/or personal care products (antacids, some mouthwashes) may contain sodium or alcohol. |
| Encourage scheduling activities with adequate rest periods. | Adequate rest decreases metabolic demands on the body and increases energy available for tissue regeneration. |
| Promote diversional activities that are enjoyable to patients. | Prevents boredom and minimizes anxiety and depression. |
| Recommend avoidance of persons with infections, especially URI. | Decreased resistance, altered nutritional status, and immune response (leukopenia may occur with splenomegaly) potentiate risk of infection. |
| Identify environmental dangers: exposure to hepatitis. | Can precipitate recurrence. |
| Instruct patient/SO of signs and symptoms that warrant notification of health care provider: increased abdominal girth; rapid weight loss/gain; increased peripheral edema; increased dyspnea, fever; blood in stool or urine; excess bleeding of any kind; jaundice. | Prompt reporting of symptoms reduces risk of further hepatic damage and provides opportunity to treat complications before they become life-threatening. |
| Instruct SO to notify health care providers of any confusion, untidiness, night wandering, tremors, or personality change. | Changes (reflecting deterioration) may be more apparent to SO, although insidious changes may be noted by others with less frequent contact with patient. |
Administering medications
| INTERVENTION | RATIONALE |
| Supplemental vitamins: vitamin K, D, and C. | Promotes prothrombin synthesis and coagulation if the liver is functional. Vitamin C deficiencies increase susceptibility of the GI system to irritation and/or bleeding. |
| Stool softeners | Prevents straining for stool with resultant increase in intra-abdominal pressure and risk of vascular rupture and hemorrhage. |
| Provide gastric lavage with room temperature and cool saline solution or water as indicated. | In the presence of acute bleeding, evacuation of blood from GI tract reduces ammonia production and risk of hepatic encephalopathy. |
| Assist with insertion and maintenance of GI tube. | Temporarily controls bleeding of esophageal varices when controlled by other means (e.g., lavage) and hemodynamic stability cannot be achieved. |
| Prepare for surgical procedures: direct ligation (banding) or varices, esophagogastric resection, splenorenal-portacaval anastomosis. | May be needed to control active hemorrhage or to decrease portal and collateral blood vessel pressure to minimize risk of recurrence of bleeding. |
Nursing Notes
Causes
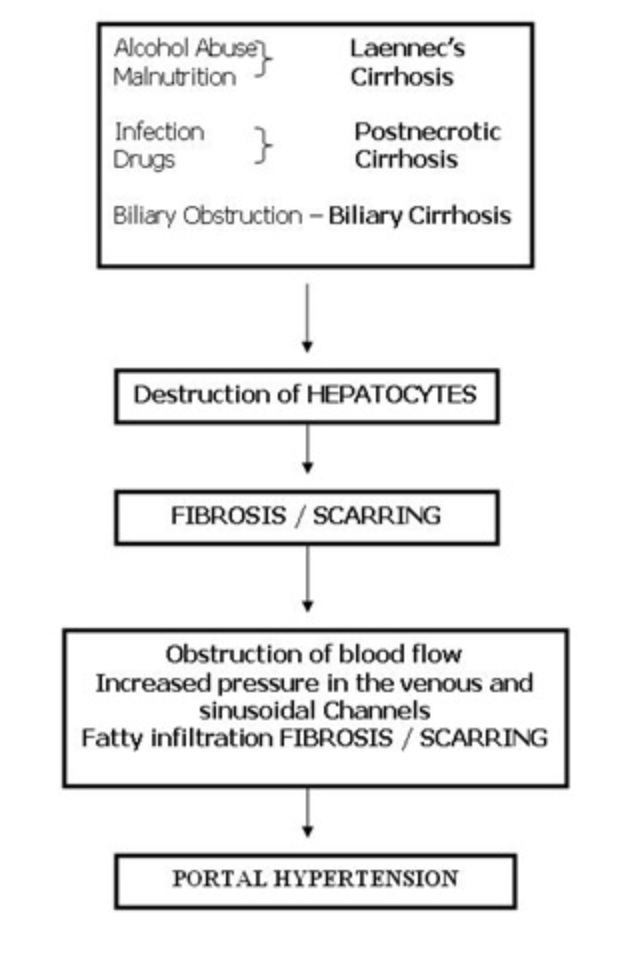
Pathophysiology

Assessment
- Early complaints including fatigue, anorexia, edema of the ankles in the evening, epistaxis, bleeding gums, and weight loss.
- In later disease:
- Chronic dyspepsia, constipation and diarrhea.
- Esophageal varices; dilated cutaneous veins around umbilicus (caput medusa); internal hemorrhoids, ascites, splenomegaly.
- Fatigue, weakness, and wasting caused by anemia and poor nutrition.
- Deterioration of mental function.
- Estrogen-androgen imbalance causing spider angioma and palmar erythema; menstrual irregularities in women; testicular and prostatic atrophy, gynecomastia, loss of libido, and impotence in men.
- Bleeding tendencies and hemorrhage.
- Enlarged, nodular liver.
Diagnostic Evaluation
- Elevated serum liver enzyme levels, reduced serum albumin.
- Liver biopsy detects cell destruction and fibrosis of hepatic disease.
- Liver scan shows abnormal thickening and a liver mass.
- CT scan determines the size of the liver and its irregular nodular surface.
- Esophagoscopy determines the presence of esophageal varices.
- Percutaneous transhepatic cholangiography differentiates extrahepatic from intrahepatic obstructive jaundice.
- Paracentesis examines ascitic fluid for cell, protein, and bacteria counts.
Primary Nursing Diagnosis
- Fluid volume excess related to retention
Therapeutic Intervention / Medical Management
Medical management is based on presenting symptoms.
- Treatment includes antacids, vitamins, balanced diet, and nutritional supplements; potassium-sparing diuretics (for ascites); avoidance of alcohol.
- Colchicine may increase the length of survival in patients with mild to moderate cirrhosis.
Surgical Intervention
- Transjugular intrahepatic portosystemic shunt may be performed in patients whose ascites prove resistant. This percutaneous procedure creates a shunt from the portal to systemic circulation to reduce portal pressure and relieve ascites.
- Orthotopic liver transplantation may be necessary.
Pharmacologic Intervention
- Provide asymptomatic relief measures such as pain medications and antiemetics.
- Diuretic therapy, frequently with spironolactone, a potassium-sparing diuretic that inhibits the action of aldosterone on the kidneys.
- I.V albumin to maintain osmotic pressure and reduce ascites.
- Administration of lactulose or neomycin through a nasogastric tube or retention enema to reduce ammonia levels during periods of hepatic encephalopathy.
Nursing Intervention
- Observe stools and emesis for color, consistency, and amount, and test each one for occult blood.
- Monitor fluid intake and output and serum electrolyte levels to prevent dehydration and hypokalemia, which may precipitate hepatic encephalopathy.
- Maintain some periods of rest with legs elevated to mobilize edema and ascites. Alternate rest periods with ambulation.
- Encourage and assist with gradually increasing periods of exercise.
- Encourage the patient to eat high-calorie, moderate protein meals and supplementary feedings. Suggest small, frequent feedings.
- Encourage oral hygiene before meals.
- Administer or teach self-administration of medications for nausea, vomiting, diarrhea or constipation.
- Encourage frequent skin care, bathing with soap, and massage with emollient lotions.
- Keep the patient’s finger nails short to prevent scratching from pruritus.
- Keep the patient quiet and limit activity if signs of bleeding are evident.
- Encourage the patient to eat foods high vitamin C content.
- Use small gauge needles for injections and maintain pressure over injection site until bleeding stops.
- Protect from sepsis through good handwashing and prompt recognition and management of infection.
- Pad side rails and provide careful nursing surveillance to ensure the patient’s safety.
- Stress the importance of giving up alcohol completely.
- Involve the person closest to the patient, because recovery usually is not easy and relapses are common.
Documentation Guidelines
- Physical findings: Bleeding, abdominal enlargement, weight gain or loss, fluid intake and output, easy respirations, breath sounds, heart sounds, level of consciousness ,gastrointestinal status (nausea ,vomiting, anorexia, diarrhea) ,color of skin and sclera
- Laboratory results: White blood cell count, hemoglobin and hematocrit, albumin, serum electrolytes, ALT ,AST
- Nutrition: Tolerance of diet, appetite, ability to maintain body weight
- Response to treatment: Medications, surgery, paracentesis
Discharge and Home Healthcare Guidelines
- ALCOHOL ABUSE TREATMENT. Emphasize to the patient with alcoholic liver cirrhosis that continued alcohol use exacerbates the disease. Stress that alcoholic liver disease in its early stages is reversible when the patient abstains from alcohol. Encourage family involvement in alcohol abuse treatment. Assist the patient in obtaining counseling or support for her or his alcoholism.
- FOLLOW-UP. Encourage the patient to seek frequent medical follow-up. Visits from a community health nurse to monitor the patient’s progress and to help with any questions or problems at home are also helpful.
- SUPPORT GROUPS. Refer the patient to an alcohol support group or liver transplant support group.