
Nervous System
The nervous system is central to maintaining homeostasis in the body [in conjunction with the endocrine system]. The following critical organs comprise the nervous system: the brain, spinal cord, nerves, and ganglia. The nervous system affects all aspects of one’s health, like mental activity, mobility, heart and respiration rates, sleep, among many others. Its general functions can be thought of as three-fold: sensory, integrative, and motor.
Embryonic Development of the Nervous System
Introduction
The general embryonic development can be described in 2 ways
Trimesters (3x 3-month periods)
- First → foundations of major organs
- Second → development of organs
- Third → rapid growth & fully functional organs
Anatomical stages
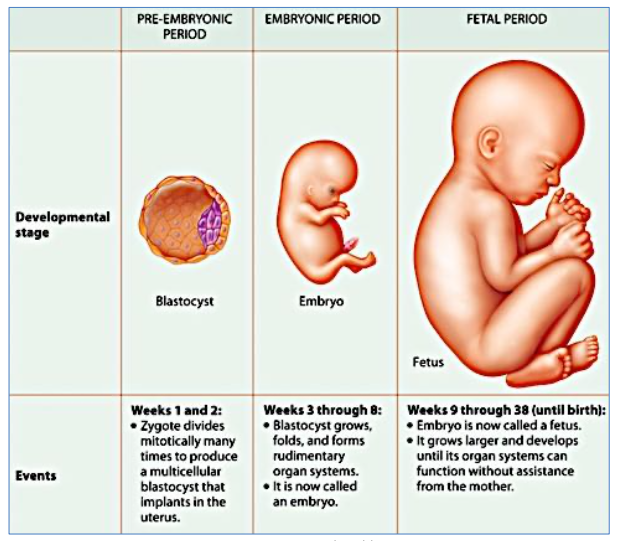
- Pre-embryonic period (0-2 weeks)
- Fertilization
- Blastocyst formation & explanation
- Gastrulation
- Embryonic period (3-8 weeks)
- Development and differentiation of 3 germ layers into foundations of organs
- Fetal period (9 weeks to birth)
- Period of growth, not differentiation
Some useful terminology
| rostral | head |
| caudal | tail |
| dorsal | back |
| ventral | front |
| ganglia | groups of nerve cell bodies |
| gyrus | elevations (crests) of the folds on the cerebral cortex |
| sulcus | grooves (furrows) between gyri on the cerebral cortex |
Embryonic development of the nervous system
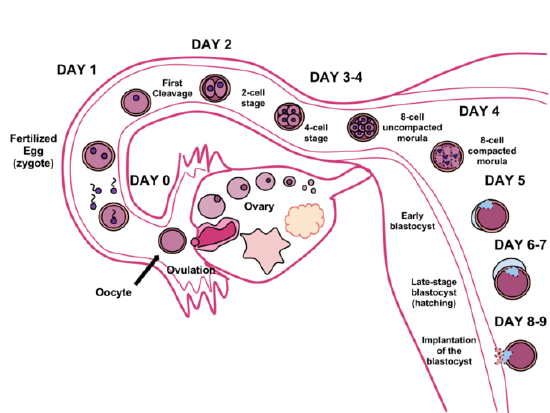
Blastocyst (pre-embryonic period)
- A fertilized egg reaches the Morula stage (Day 3), differentiates into a Blastocyst (Day 7) and then implants in the endometrium
- The implanted Blastocyst consists of an ‘inner-cell mass’ surrounded by Trophoblasts
- This ‘inner-cell mass’ differentiates to form the Bilaminar Disc (2 layers of cells)
- Epiblast layer: The top layer of columnar cells
- Hypoblast layer: The bottom layer of cuboidal cells

Gastrulation (Embryonic Period, week 3+)
- Gastrulation is the process that establishes the 3 primary germ layers in the embryo
- Begins with formation of the primitive streak (a shallow midline groove) along the caudal/tail half of bilaminar disc
- At the cephalic/head end of the primitive streak is the primitive node which surrounds the small primitive pit. Cells of the epiblast proliferate & migrate through the primitive pit into the gap between the epiblast & the hypoblast. This is known as invagination
- The epiblast then becomes the ectoderm, the invaginated cells become the mesoderm and the hypoblast becomes the endoderm
Neurulation
- Neurulation is the process wherein the ectoderm around the midline thickens to form an elevated neural plate
- This neural plate invaginates to form a neural groove down the midline, flanked by two neural folds
- The notochord, a flexible rod of mesoderm-derived cells, defines the primitive axis of the embryo
- The outer edges of the two neural folds continue folding towards the midline where they fuse together to form the neural tube
- Initially this happens around the center of the embryo, leaving open neural grooves at both the cephalic & caudal ends
- These neural grooves (aka neuropores), close off by around week 6 of development
- Failure of a neuropore to close can result in neural tube defects such as spina bifida
- The hollow part inside the neural tube is called the neurocoele
- The neural tube then separates from the ectoderm and sinks down to the level of the mesoderm
- The mesoderm that flanks the sunken neural tube develops into the somites, which eventually become the skin, skeletal muscle, and vertebrae & skull
- Next, some cells on the top of the neural tube differentiate and separate to form the neural crest
- Cells of the neural crest eventually migrate & give rise to peripheral sensory neurons, autonomic neurons, and sensory ganglia of the spinal nerves
Somites
- Somites are the mesoderm tissue directly adjacent to neural tube
- Somites grow in association with the developing nervous system → establish early connections
- Somites differentiate into 3 regions:
- Sclerotome becomes the vertebral column & skull
- Myotome becomes skeletal muscle
- Dermatome becomes skin
- Hence, the somites determine the distribution of nervous supply to all mesoderm-derived tissue

Development of the neural tube into the spinal cord
Once the neural tube closes, the cells differentiate into neuroblasts
- These neuroblasts give rise to 2 concentric layers, the mantle layer (inner) and the marginal layer (outer)
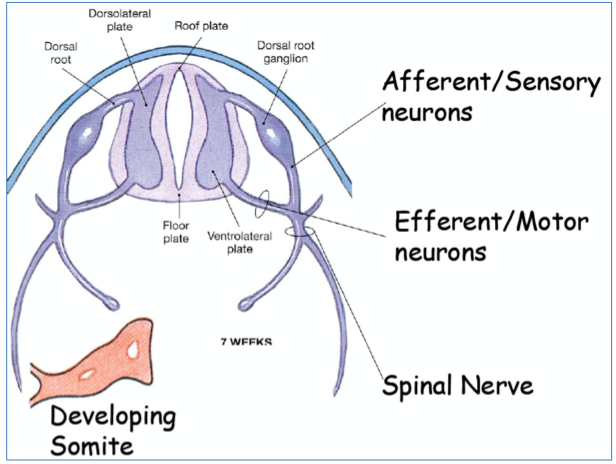
- Mantle layer: later forms the gray-matter of the spinal cord (ventral & dorsal ‘horns’)
- Marginal layer: later forms the white-matter of the spinal cord
- The dorsal & ventral regions of the mantle layer thicken forming 2 basal plates, and 2 alar plates
- Basal plates: (motor plates) develop into motor neurons innervating skeletal muscles
- Become the ventral horns
- Alar plates: (sensory plates) develop into sensory neurons
- Become the dorsal horns
- Basal plates: (motor plates) develop into motor neurons innervating skeletal muscles
Note: the lateral horns in the thoracic & lumbar regions of the spinal cord are autonomic motor neurons and their axons exit via the ventral roots.

Development of the neural crest cells into the sensory (‘dorsal-root’) ganglia of PNS
- Neural crest cells also differentiate into neuroblasts which become the sensory (‘dorsal-root’) ganglia
- The neuroblasts of the dorsal-root ganglia develop 2 processes:
- Penetrates into the alar plate of the neural tube and/or into the marginal layer & up to brain
- Grows distally (outwards) and integrates with the ventral motor root, forming the trunk of the spinal nerve (these neurons eventually terminate in the sensory receptors in skin/muscle/tendons)
Note: these dorsal-root ganglia processes form the ‘sensory pseudounipolar’ nerve-type.

By week 7, we have a near functional nervous system very similar in organization to adult anatomy.
Development of the head & brain
Neural tube enlargement (cephalic end)
- At around 3-4 weeks, the cephalic portion of the neural tube enlarges to form 3 regions, the primary brain vesicles:
- Prosencephalon (forebrain)
- Mesencephalon (midbrain)
- Rhombencephalon (hindbrain)
Note: the cephalic flexure between the prosencephalon & mesencephalon – important in humans for bipedalism (brain at 90 degrees to spinal cord)
- By around 4-5 weeks, the primary brain vesicles develop further:
- Prosencephalon (forebrain) develops into:
- Telencephalon (future cerebral hemispheres)
- Diencephalon (future thalamus & hypothalamus)
- Prosencephalon (forebrain) develops into:
Mesencephalon (midbrain)
- Rhombencephalon (hindbrain) develops into:
- Metencephalon (future pons & cerebellum)
- Myelencephalon (future medulla)

Brain formation
- At around 11-13 weeks, there is massive proliferation of neuroblasts in cephalic neural tube, causing folding due to lack of space within the cranium

Pharyngeal arches & cranial nerves
- Pharyngeal arches are similar to the somites in lower parts of the embryo
- Each pharyngeal arch consists of:
- Ectoderm tissue → cranial nerves & skin of face
- Mesenchyme (mesoderm) tissue → musculature of face & neck
- Endoderm tissue → pharyngeal epithelium
- Note: essentially, this results in segmental development of the head & neck, similar to somites.

Formation of ventricles
- The neurocoele of the neural tube becomes the ventricles of the adult brain
- Lateral ventricles (ventricles 1 & 2)
- Sits in the cerebral hemispheres (telencephalon)
- Are shaped due to folding of brain during development
- Each consists of:
- A frontal (anterior) horn
- A ‘body’
- An occipital (posterior) horn
- A temporal (inferior) horn
- Third ventricle
- Sits in the diencephalon
- Lateral walls formed by thalamus & hypothalamus
- Connects with the 4th ventricle via the cerebral aqueduct
- Fourth ventricle
- Sits in the brainstem
- Is continuous with the spinal canal (central canal)
- Lateral ventricles (ventricles 1 & 2)


Overview & Organization of the Nervous System
Overview
Macrostructures
- Brain
- Spinal cord
- Peripheral nerves
- Sense organs
- Eyes
- Ears
- Tongue
- Olfactory bulbs
- Skin
Functions
- Detection of stimuli (external/internal)
- Response to stimuli
- Coordinates activity of other organs & systems
Organization of the nervous system
Central nervous system (the “CPU” and “motherboard”)
- Brain
- Spinal cord
Peripheral nervous system (the “cables)
- Cranial nerves and spinal nerves
- Communication between CNS and rest of the body

The neuron: structural features
- Receptive field: dendrites
- Stimulated by inputs
- Cell body: soma
- Responds to graded inputs
- Efferent projection: axon (and axon hillock)
- Conducts nerve impulses to target
- Myelinated and unmyelinated
- Efferent projection: myelin sheath
- Efferent projection: “nodes of Ranvier”
- Output: synaptic terminals (axon terminals)

Supporting cells: neuroglia (glia)
- Smaller support cells of NS
- Outnumber neurons 10:1
- Structural & mechanical support
- Roles in maintaining homeostasis & myelination
- Immune responses via phagocytosis
Neuroglia of the central nervous system (CNS)
Astrocytes
- Nutrient bridge between neuron & capillaries
- Guide migrating young neurons
- Synapse formation
- Mop up excess K+ ions & neurotransmitters
Microglia
- Long thorny processes
- Monitors neuron health
- Senses damaged neurons
- Migrates to damaged neuron
- Phagocytoses microbes and debris (immune cells are denied access to CNS)
Oligodendrocytes
- Myelin formation in CNS
Ependymal cells
- Lines central cavities of brain and spinal cord
- Blood-brain barrier
- Beating cilia circulates cerebrospinal fluid (CSF)
Neuroglia of the peripheral nervous system (PNS)
Schwann cells
- Myelin formation → wrap around axon
- Regeneration of damaged neurons
Satellite cells
- Surround neuron bodies
- Structure, nutritional support, protection

Connective tissue sheaths on peripheral nerves
Endoneurium
- Delicate connective tissue layer
- Surrounds each axon
Perineurium
- Coarser connective tissue layer
- Bundles groups of fibers into fascicles
Epineurium
- Tight, fibrous sheath
- Bundles fascicles into a single nerve
- Houses blood vessels

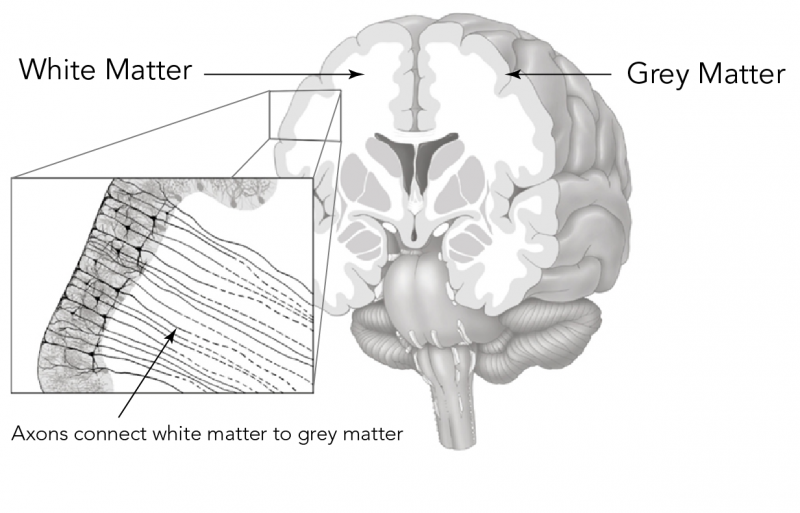
Gray matter and white matter
Gray matter
- Made up of neuron bodies (soma)
- Imbedded in neuroglial cells
- Examples
- Cortex of brain
- Center of spinal cord
- Ganglia/nuclei
White matter
- Neuron fibers (axons & dendrites)
- White due to myelin
- Examples
- Peripheral nerves & plexuses
- Central fiber tracts

Ganglia
- Collections of neuron cell bodies in the PNS
- Afferent spinal nerves
- Cell bodies of sensory neurons
- ‘Dorsal root ganglion’
- Efferent spinal nerves
- Cell bodies of autonomic nerve fibers
- ‘Sympathetic trunk ganglion’
- In central nervous system
- Called: basal nuclei/nuclei
- Important for both motor & autonomic nervous systems
- Afferent spinal nerves

Spinal nerves
Dermatomes
A portion of the mesoderm (skin, sensory receptors, sebaceous glands, blood vessels) innervated by the cutaneous branches of a single spinal nerve


Surface Anatomy of the Brain
Surface anatomy
Dorsal landmarks
Fissures
- Longitudinal fissure separates left & right hemispheres
- Transverse cerebral fissure separates occipital lobe from cerebellum
Sulci
- Central sulcus separates the frontal & parietal lobes
- Lateral sulcus separates the temporal lobe from the other lobes
- Parieto-occipital sulcus separates parietal lobe & occipital lobe
Lobes
- Occipital lobe is the most caudal lobe (visual cortex)
- Temporal lobe is the most lateral lobe
- Frontal lobe is the most anterior lobe

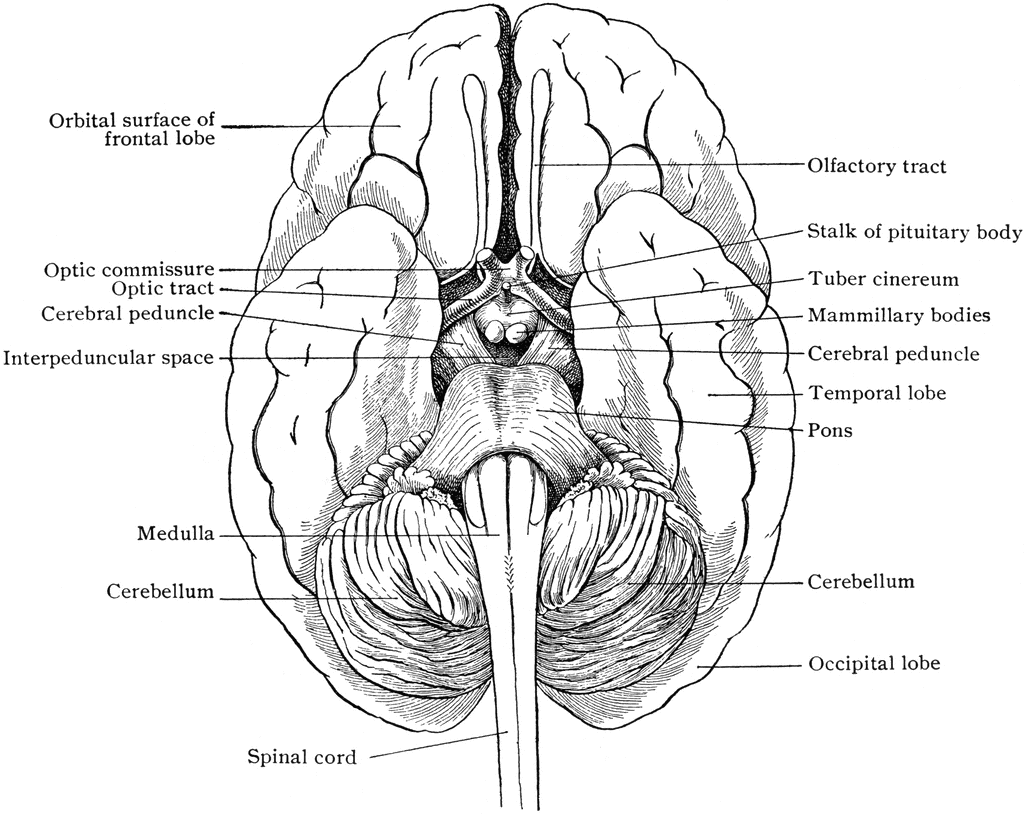
Ventral landmarks
- Olfactory bulbs are responsible for sense of smell
- Optic chiasm (“optic crossing”) is an ‘X’-shaped crossing-over of optic nerves
- Infundibulum is the connection between pituitary & hypothalamus
- Hypothalamus is responsible for many autonomic homeostatic functions
- Pituitary is an important neuroendocrine organ
- Mamillary bodies form part of the limbic system & are important for recollective memory
- Pyramids (pyramidal tracts) carry motor fibers from the cerebral cortex to the spinal cord
Medial landmarks (i.e., on sagittal section)
- Cingulate gyrus is part of the limbic system and is involved in emotion and behavior regulation
- Corpus callosum is a thick bundle of connecting nerve fibers connecting left and right hemispheres
- Lateral ventricle holds cerebrospinal fluid
- Pineal body is involved in circadian rhythm (night/day body clock)
- Thalamus has multiple physiological roles including sensory, motor, & consciousness regulation
- Hypothalamus regulates hunger, thirst, temperature control, memory, & stress responses
- Pituitary gland controls metabolism, growth, sexual function, blood pressure, and others
- Colliculi are nestled in between the cerebrum & cerebellum
- 2x superior → controls eye movements
- 2x inferior → part of auditory pathway
- Cerebellum is important for coordination, precision, & timing of movements
- Pons are critical for respiratory rhythm & breathing
- Medulla oblongata relays messages between the brain and spinal cord; also regulates cardiorespiratory functions
- Fourth ventricle contains CSF

Coronal section landmarks
- Cortex (gray matter) has key roles in attention, perception, awareness, thought, memory, language, sensation, and motor functions
- White matter is mostly axons & myelin; relays action potentials to their destinations
- Lateral ventricle contains CSF
- Caudate nucleus is important in planning & executing movement; also has learning, memory, reward, motivation & emotional functions
- Corpus striatum is the reinforcement circuit of the brain
- Thalamus has multiple physiological roles including sensory, motor, and consciousness regulation
- Massa intermedia is the bridge between the left & right thalamus
- Hippocampus plays major role in learning and memory

Blood Supply of the Brain
Why does the brain need blood?
- Consumes 15-20% of the body’s total energy needs and receives 15% of cardiac output, despite being only 2% of total body mass
- Neurons require high ATP to
- Maintain ion gradients across plasma membrane
- Regulate neurotransmitter synthesis/re-uptake
- Neurons have no anaerobic capacity → therefore the brain absolutely depends on oxygenated blood
- Hence, any deficit in blood supply is detrimental (≈30+ seconds of a lack of blood/O2 to brain → unconscious)
Blood supply to the brain is an anastomosis
- Anastomosis is where multiple arteries supply the same region of tissue (i.e., a dual blood supply)
- The advantage → if one of the arteries becomes blocked/damaged, the other will compensate for it
Arterial supply of the brain
- Brain is supplied by 2 arterial systems
- 2x vertebral arteries → 1x basilar artery → Circle of Willis
- 2x internal carotid arteries → Circle of Willis
- Circle of Willis, the anastomosis of the brain
- The ‘roundabout’ of arteries on the underside of the brain with multiple ‘roads’ coming off it
- Encircles the optic chiasm, the pituitary gland & the mammillary bodies
- The ‘roads’: (anterior → posterior)
- 2x anterior cerebral arteries
- 1x anterior communicating artery
- 2x internal carotid arteries
- 2x middle cerebral arteries
- 2x posterior communicating arteries
- 2x posterior cerebral arteries
- 1x basilar artery
Note: Communicating arteries are always patent, but generally not functional (no blood flow) when blood flow from both carotids & basilar arteries is normal. However, if blood flow from one of the major arteries is impeded, blood is shunted through the communicating arteries to compensate.


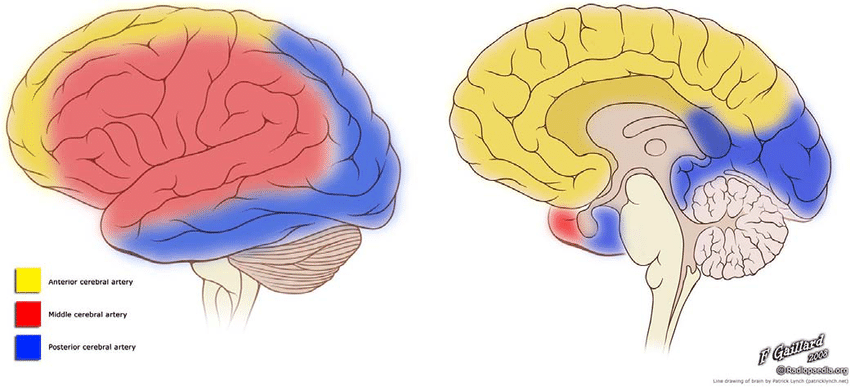
Distribution of cerebral arteries
Anterior cerebral arteries
- Travels up and over the corpus callosum, sprouting branches outwards towards the cortex
- Medial portion of frontal lobe (including cortex)
- Medial portion of parietal lobe (including cortex)
- Corpus callosum
Middle cerebral arteries
- Travels through lateral fissure/sulcus and emerges onto the lateral surface of the brain
- Lateral portion of frontal lobe (including cortex)
- Lateral portion of parietal lobe (including cortex)
- Entire temporal lobe (including cortex)
Posterior cerebral arteries
- Travels along the inferior brain surface between the cortex and the cerebellum
- Inferior portion of temporal lobe (including cortex)
- Posterior-medial portion of parietal lobe (including cortex)
- Entire occipital lobe (including cortex)
The blood-brain barrier
- Isolates the brain from blood to provide a stable environment, necessary for control & function of CNS neurons
- How?
- The endothelial cells of the CNS capillaries are seamlessly joined by tight junctions
- This prevents diffusion of most materials except dissolved gasses & lipid-soluble compounds
- Therefore, any required water-soluble compound must be transported across the BBB
- Thick basement membrane of capillary
- The endothelial cells of the CNS capillaries are seamlessly joined by tight junctions
- Note: In the 2 choroid plexuses, the BBB is formed by tight junctions between glial (ependymal) cells as the capillaries in this region are fenestrated and highly leaky
- The BBB exists everywhere, except:
- Hypothalamus → monitors chemical composition of blood (i.e., hormone levels, water balance, etc.)
- Vomiting center → monitors poisonous substances in blood

Venous drainage of the brain (via dural sinuses)
- Venous drainage begins with venous blood collecting in small venous channels known as dural sinuses
- Sinuses sit within the dura mater
- The dura mater is the thickest and outermost of the 3 meninges of the brain
- Extends deep into the brain in 2 locations, the falx cerebri and tentorium cerebelli
Falx cerebri
- The dura mater folds deep into the longitudinal fissure (falx cerebri) of the brain,
where it forms 2 sinuses
- A triangular superior sagittal sinus at the top of the dural fold
- A lower inferior sagittal sinus at the bottom of the dural fold

Tentorium cerebelli
- The dura mater folds deep into the transverse cerebral fissure (tentorium cerebelli) of the brain, where it forms a pair of sinuses
- The right and left transverse sinuses
- All the blood from the superior & inferior sagittal sinuses and the straight sinus empties into these transverse sinuses

- The left and right transverse sinuses become the left and right sigmoid sinuses, respectively
- These sigmoid sinuses turn inferiorly and become the internal jugular veins

Regulation of blood flow to the brain
Blood flow to the brain is autoregulated
- i.e., blood pressure in the brain is kept constant, despite systemic blood pressure fluctuations
- It also means different areas of the brain control their blood flow depending on metabolic activity
The myogenic autoregulation of blood flow to the brain
- When mean arterial pressure rises, the SNS constricts the larger arteries of the brain to prevent damaging high pressures in smaller, more delicate vessels (important for preventing stroke)
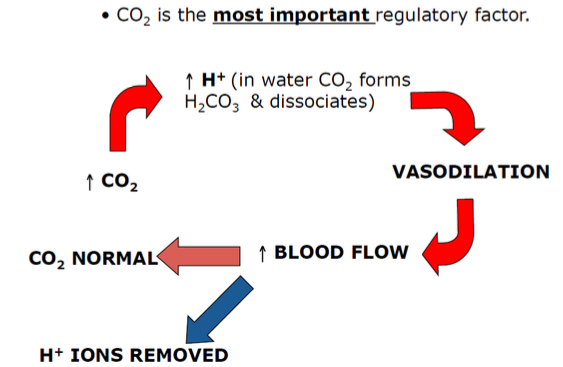
The 3 metabolic autoregulatory factors affect blood flow to the brain
Blood
- ↑[CO2] → Vasodilation (to ↑ Blood Flow)
- ↓[CO2] → Vasoconstriction (to ↓ Blood Flow)
Blood/CSF pH
- ↑[CO2] → ↑[H+] via carbonic anhydrase → ↓pH → Vasodilation (to ↑ Blood Flow)
- ↓[CO2] → ↓[H+] via carbonic anhydrase → ↑pH → Vasoconstriction (to ↓ Blood Flow)
Blood/CSF [O2]
- ↓[O2] → Vasodilation (to ↑ Blood Flow)
- ↑[O2] → Vasoconstriction (to ↓ Blood Flow)
Intracranial pressure
What is it?
Pressure within the cranium created by CSF, and exerted on the brain tissue and brain’s blood circulation vessels
Determinants
- CSF production/resorption (e.g., ↑Production + ↓Resorption)
- Brain tissue (e.g., tumor/inflammation)
- Blood (e.g., hemorrhage)
High intracranial pressure
- Compresses cerebral arteries → decreased blood supply → brain drainage
- Can also displace the brain
Symptoms of high intracranial pressure
- Altered consciousness
- Changes in BP & HR
- Changes in eye responses
- Changes in motor function
Cerebral blood flow and intracranial pressure
- Cerebral blood flow is carefully regulated under normal conditions
- Cerebral blood flow
- What percentage of cardiac output goes to the cerebral circulation at rest?
- 750 mL/min (15% of CO)
- Relationship between cerebral blood flow & arterial pressure
- What percentage of cardiac output goes to the cerebral circulation at rest?

- Kelly-Monroe Doctrine
- States that the cranial compartment is incompressible, and the volume is fixed
- The cranial constituents (blood, CSF, and brain matter) create a state of volume equilibrium:
- Any increase in volume of one of the constituents must be compensated by a decrease in volume of another
- Volume buffers
- Both CSF and, to a lesser extent, blood volume
- e.g. an extradural hematoma → CSF & venous blood volumes are decreased
- → maintain normal ICP
- Buffer capacity ≈ 100-120 mL
Flow & production of CSF

Reabsorption of CSF into the dural sinuses
- Note: CSF is constantly being produced, and therefore must also be constantly drained to prevent a rise in intracranial pressure
- Therefore, CSF is reabsorbed into the venous system via diffusion through arachnoid villi (arachnoid granulation)
- Arachnoid villi are invaginations of arachnoid mater through the dura mater and into the superior sagittal sinus

Cerebral edema
What is it?
An excess accumulation of water in the intracellular and/or extracellular spaces of the brain
Types of cerebral edema
Vasogenic
- Extracellular edema
- Due to a breakdown of tight endothelial junctions which form the BBB
- e.g., hydrostatic cerebral oedema – where acutely high cerebral capillary pressure results in fluid moving from capillary → ECF
Cytotoxic
- Intracellular edema
- Due to a defect in cellular metabolism → inadequate functioning of the Na/K-ATPase in the cell membrane → cellular retention of H2O
Osmotic
- Extracellular edema
- Where a drop in plasma osmolality (compared to CSF osmolality) causes water to flow from the venous sinuses back into the subarachnoid space
Migraines
What are they?
Incapacitating neurovascular disorder characterized by unilateral, throbbing headaches, photophobia, phonophobia, nausea, & vomiting
What causes them?
Decrease in serotonin levels → ↑sensitivity to migraine triggers + cerebral vasoconstriction → ↓cerebral blood flow → raphe nuclei in brainstem release serotonin → cerebral vasodilation + release of proinflammatory mediators from trigeminal nerve & spinal nerves → perivascular cerebral inflammation → pain
Classic vs. common
Classic
Associated with ‘aura’ (a visual symptom, such as an arc of sparkling/scintillating zig-zag lines or blotting out of vision, or both)
Common
Migraine without ‘aura’ (only 20% of sufferers experience aura; most bypass aura phase)
Migraine as a risk factor
- ↑ Risk of silent posterior cerebral infarcts
- ↑ Risk of stroke & CVD (women)
- ↑ Risk of MI (men)
Cranial Nerves
Similarities between spinal nerves & cranial nerves
Cranial nerves develop similar to spinal nerves, and hence have a similar structural organization
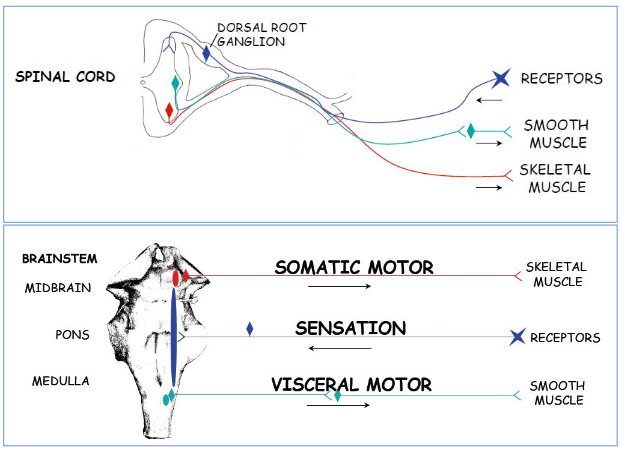
Sensory cranial nerves
Similar to afferent spinal nerves – sensory cranial nerves’ dendrites are associated with peripheral sensory receptors & their cell bodies are located in a sensory ganglia (similar to the dorsal root ganglion in the spinal cord). Their axons then terminate in the sensory nuclei of the brainstem (similar to dorsal horn of spinal cord), and synapse with one of the ascending pathways (depending on the type of stimulus):
- Touch → posterior pathway
- Pain → spinothalamic
- Proprioception → spinocerebellar
Somatic motor cranial nerves
Similar to efferent spinal nerves – motor cranial nerves (both somatic & branchial) have
their cell bodies in gray-matter motor nuclei in the brainstem (similar to ventral horn of
spinal cord). Their axons leave the brainstem & directly innervate the skeletal muscles.
Visceral motor cranial nerves
Similar to autonomic spinal nerves – visceral-motor cranial nerves have their cell bodies in the gray-matter visceral nuclei in the brainstem (similar to lateral horn of spinal cord). Their axons then synapse with a second-order neuron in an autonomic ganglion, where the second neuron innervates the smooth muscle
e.g., just as spinal nerves grow in association with their somites, some cranial nerves grow in association with the 6 pharyngeal arches
The pharyngeal (branchial) arches
- Note: There are 6 pharyngeal arches, but the 5th only exists transiently during embryonic growth
- No structures result from the 5th arch
- Appear ≈4-5 weeks of development
| Pharyngeal arch | Nerve | Muscular contributions |
| 1st – Mandibular | Trigeminal (CN V) | Muscles of mastication Anterior digastricMylohyoidTensor tympani Tensor veli palatini |
| 2nd – Hyoid | Facial (CN VII) | Muscles of facial expression Posterior digastricStylohyoidBuccinator |
| 3rd | Glossopharyngeal (CN IX) | Stylopharyngeus |
| 4th | Vagus (CN X) | Cricothyroid muscleSoft palate muscles |
| 6th | Vagus (CN X) | Intrinsic laryngeal muscles |

The 12 cranial nerves: basic overview
- Olfactory
smell
- Optic
vision (visual acuity)
- Oculomotor (‘eye-mover’)
controllers 4 of the 6 eye muscles
- Trochlear (pulley)
controls 1 of the extrinsic eye muscles (pulley-shaped)
- Trigeminal
3-branched (ophthalmic, maxillary, mandibular) sensory fibers to the face & cornea + mastication
- Abducens (‘abduct)
controls extrinsic eye muscle that abducts the eyeball (lateral rotation)
- Facial
facial expression (i.e., furrow brow, shut eyes, smile, etc.)
- Vestibulocochlear
hearing and balance (formerly the ‘auditory nerve’)
- Glossopharyngeal (‘tongue & pharynx’)
sensory tongue & pharynx (gag reflex)
- Vagus (‘the wanderer’)
mouth motor + parasympathetic effects in the thorax & abdomen
- Accessory
neck & shoulder muscles
- Hypoglossal (‘under-tongue’)
tongue movement – poke tongue out

Functional components of cranial nerves
Cranial nerves carry one/more of the following 5 functional components
| Voluntary (somatic) motor Somatic motor: “general somatic efferents” (GSE) – Innervate striated skeletal muscle derived from embryonic somites, not pharyngeal arches – Including ocular muscles, tongue, external neck muscles (sternocleidomastoid & trapezius) Branchial motor: “special visceral efferents” (SVE) – Innervate striated skeletal muscle derived from embryonic pharyngeal arches – Including muscles of the face, palate, pharynx, larynx, mastication |
Oculomotor Trochlear Trigeminal Abducens Facial Glossopharyngeal Vagus Accessory Hypoglossal |
| Involuntary (visceral) motor: “general visceral efferents” (GVE) – Innervate smooth muscle in vessels/glands/etc. via a 2-neuron approach Presynaptic fibers emerge from the brain as cranial nerves, which then synapse in a parasympathetic ganglion Postsynaptic neurons then innervate the smooth muscles & glands, etc. – Constitute the cranial outflow of the parasympathetic nervous system |
Oculomotor Facial Glossopharyngeal Vagus |
| Visceral sensation: “general visceral afferents” (GVA) Blood pressure, blood O2/CO2 from carotid sinus and body, plus visceral sensation from pharynx, larynx, trachea, bronchi, lungs, heart, GI tract |
Oculomotor Trigeminal Facial Glossopharyngeal Vagus |
| Special sensation: “special somatic/visceral afferents” (SSA/SVA) Vision, taste, smell, hearing, balance |
Olfactory Optic Facial Vestibulocochlear Vagus |
| Nerve | Functional components | Location of nerve cell bodies | Cranial exit point | Major functions |
| CN I | Special sensory | Olfactory epithelium | Cribriform plate of the ethmoid bone | Smell |
| CN II | Special sensory | Retinal ganglion | Optic canal | Vision and associated reflexes |
| CN III | Somatic motor | Midbrain | Superior orbital fissure | Movements of eyes (superiorly, inferiorly, medially) |
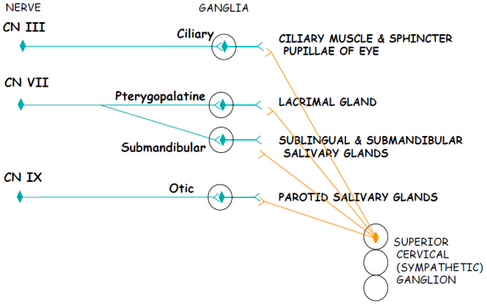
| CN III | Visceral motor (parasympathetic) | Presynaptic – midbrain, postsynaptic – ciliary ganglion | Superior orbital fissure | Pupillary constriction and lens accommodation (parasympathetic) |
| CN IV | Somatic motor | Midbrain | Superior orbital fissure | Movements of eyes (inferolaterally) |
| CN V1 | General sensory | Trigeminal ganglion | Superior orbital fissure | Sensation from cornea, V1 dermatome |
| CN V2 | General sensory | Pons | Foramen rotundum | Sensation from maxillary teeth, nasal mucosa, maxillary sinuses, palate, V2 dermatome |
| CN V3 | General sensory | Pons | Foramen ovale | Sensation from mandibular teeth, mucosa of mouth, tongue, V3 dermatome |
| CN V3 | Branchial motor | Pons | Foramen ovale | Muscles of mastication, swallowing |
| CN VI | Somatic motor | Pons | Superior orbital fissure | Lateral rectus muscle – abduction (lateral rotation) of the eye |
| CN VII | Branchial motor | Pons | Internal acoustic meatus; facial canal; stylomastoid foramen | Facial muscles, some muscles of mastication |
| CN VII | Special sensory | Geniculate ganglion | Internal acoustic meatus; facial canal; stylomastoid foramen | Taste (anterior ⅔ of tongue) |
| CN VII | Visceral motor (parasympathetic) | Presynaptic – pons, postsynaptic – pterygopalatine ganglion, submandibular ganglion | Internal acoustic meatus; facial canal; stylomastoid foramen | Stimulation of submandibular & sublingual salivary glands, lacrimal glands |
| CN VIII – Vestibular | Special sensory | Vestibular ganglion | Internal acoustic meatus | Position of head, balance (body’s gyro) |
| CN VIII – Cochlear | Special sensory | Spiral ganglion | Internal acoustic meatus | Hearing (via spiral organ) |
| CN IX | Branchial motor | Medulla | Jugular foramen | Stylopharyngeus muscle (assists with swallowing) |
| CN IX | Visceral motor | Presynaptic – medulla, postsynaptic – otic ganglion | Jugular foramen | Stimulate parotid salivary gland |
| CN IX | Visceral sensory | Superior ganglion | Jugular foramen | Visceral sensation from parotid gland, carotid sinus, pharynx, middle ear |
| CN IX | Special sensory | Inferior ganglion | Jugular foramen | Taste (posterior ⅓ of tongue) |
| CN IX | General sensory | Inferior ganglion | Jugular foramen | Cutaneous sensation of external ear |
| CN X | Branchial motor | Medulla | Jugular foramen | Constrictor muscles of pharynx, muscles of larynx, palate, upper ⅔ esophagus |
| CN X | Visceral motor | Presynaptic – medulla, postsynaptic – viscera | Jugular foramen | Maintains smooth muscle, tone in trachea & bronchi, peristalsis in git & ↓HR |
| CN X | Visceral sensory | Superior ganglion | Jugular foramen | Visceral sensation from base of tongue, pharynx, larynx, trachea, bronchi, heart, esophagus, stomach & intestine → L-colic flexure |
| CN X | Special sensory | Inferior ganglion | Jugular foramen | Taste (epiglottis & palate) |
| CN X | General sensory | Superior ganglion | Jugular foramen | Sensation from external ear |
| CN XI | Somatic motor | Spinal cord | Jugular foramen | Sternocleidomastoid, trapezius muscles |
| CN XII | Somatic motor | Medulla | Hypoglossal canal | Intrinsic & extrinsic muscles of the tongue |
Cranial nerve nuclei
- Location
- CN I & II – both extensions of the forebrain
- CN III to XII – originate from nuclei located in brainstem
- Organization
- Nuclei of similar functional components are generally aligned into functional columns in the brainstem
Sensory ganglia of cranial nerves
| Cranial nerve | Receptor types | Sensory ganglia |
| Olfactory | Olfactory | Olfactory epithelium |
| Optic | Retinal | Retina of the eye |
| Trigeminal | Somatosensory | Trigeminal ganglion |
| Facial | Somatosensory | Geniculate ganglion |
| Vestibulocochlear | Equilibrium and hearing | Vestibular ganglion, spiral ganglion |
| Glossopharyngeal | Somatosensory, visceral, taste | Inferior ganglion |
| Vagus | Somatosensory, visceral, taste | Superior and inferior ganglia |
Parasympathetic ganglia of cranial nerves
Cranial nerves in more detail
Olfactory
- Function
- Purely special sensory
- Carry afferent impulses of smell
- Origin and course
- Olfactory nerves arise from olfactory receptors in the olfactory epithelium
- They pass up through the cribriform palate of the ethmoid bone, synapse with olfactory bulb
- Olfactory bulb neurons run posteriorly as the olfactory tract, terminates in primary olfactory cortex

Optic
- Function
- Purely sensory
- Carry afferent impulses of vision
- Origin and course
- Fibers arise from the retina, form the optic nerve
- Optic nerve passes through the optic canal of the orbit
- Optic nerves converge to form the optic chiasma where half of each nerve’s fibers cross over and continue on as optic tracts
- Optic tracts synapse in the thalamus, and thalamic fibers extend to the visual cortex


Oculomotor
- Function
- Somatic motor
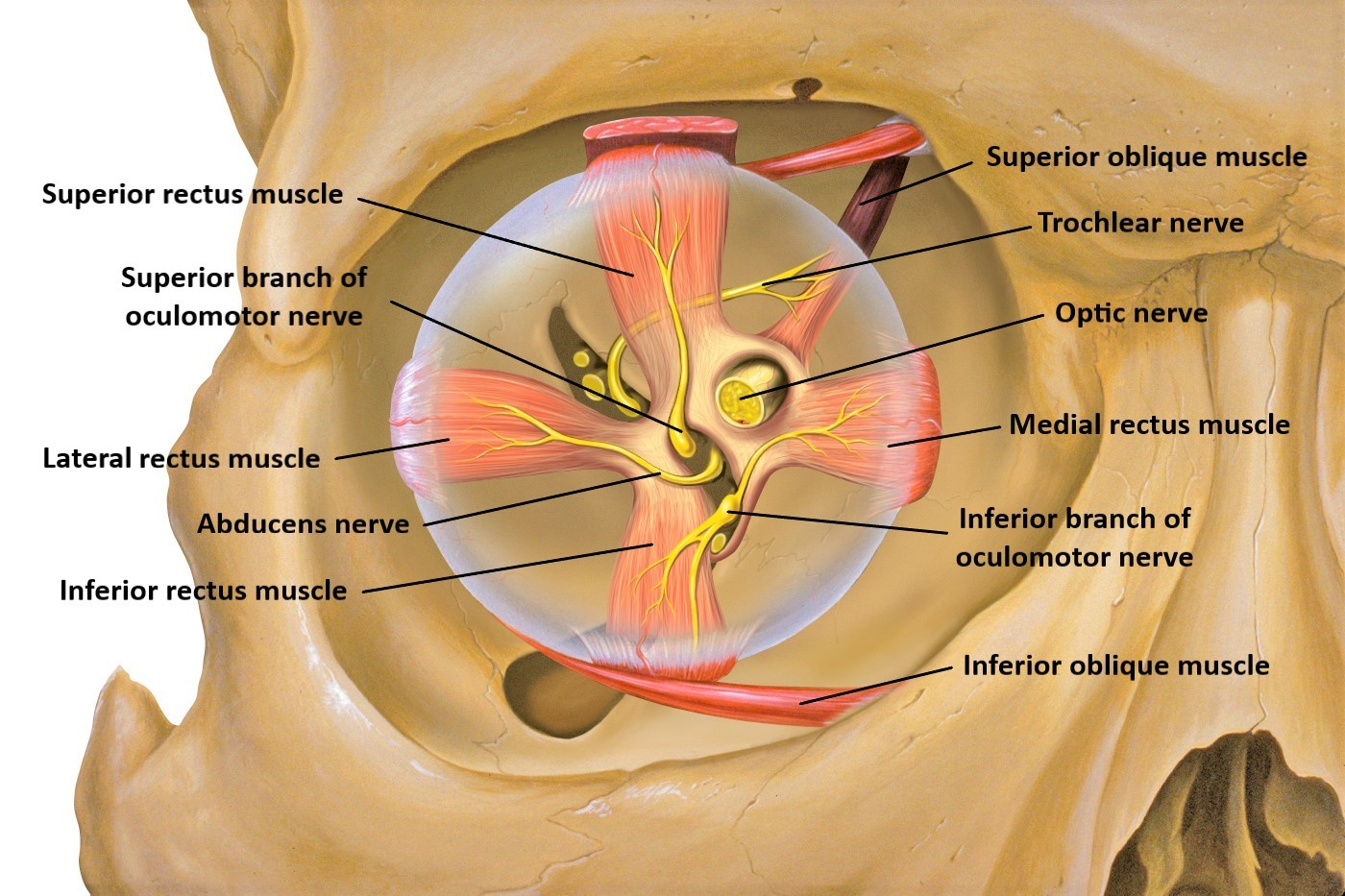
- voluntary movement of 4 of the 6 of the extrinsic eye muscles
- Inf. oblique, sup. rectus, inf. rectus, med. rectus & upper-eyelid muscle
- Note: proprioceptive afferents exist for each muscle.
- voluntary movement of 4 of the 6 of the extrinsic eye muscles
- Visceral motor
- Parasympathetic control of pupillary sphincter (constriction) & ciliary muscle (lens accommodation)
- Somatic motor
- Origin and course
- Fibers arise from the midbrain and pass through the superior orbital fissure to the eye
Trochlear
- Function
- Purely somatic motor
- voluntary movement of 1 of the 6 extrinsic eye muscles (the superior oblique)
- Purely somatic motor
- Origin and course
- Fibers arise from the midbrain, pass through superior orbital fissure to the eye
Trigeminal
Note: Has 3 divisions (ophthalmic, maxillary, mandibular), each with different specific functions and courses through the skull
- Function
- Mostly somatosensory (From face)
- Some branchial motor
- Origin and course
- Ophthalmic – fibers run from face → superior orbital fissure → pons
- Maxillary – fibers from from face → foramen rotundum → pons
- Mandibular – fibers pass through foramen ovale
| Ophthalmic (V1) | Maxillary (V2) | Mandibular (V3) | |
| Origin & course | Fibers from face to pons via orbital fissure | Fibers run from face to pons via foramen rotundum | Fibers pass through skull via foramen ovale |
| Function | Conveys sensory impulses from skin of anterior scalp, upper eyelid, and nose; from nasal cavity mucosa, cornea, lacrimal gland | Conveys sensory impulses from nasal cavity mucosa, palate, upper teeth, skin of cheek, upper lip, lower eyelid | Conveys sensory impulses from anterior tongue (ex. taste buds), lower teeth, skin of chin, temporal region of scalp; supplies motor fibers to, and carries proprioceptor fibers from muscles of mastication |

Spinal Cord
General information
- Extends from foramen magnum
- Resides in the vertebral canal
- Bathed in cerebrospinal fluid
- Terminates at the ‘conus medullaris’ (cone of medulla) – approx l1 in adults.
- Transmits motor information distally from the brain
- Transmits sensory information back up to the brain
- Emits spinal nerves at the level of each vertebrae.
- Cauda equina
- Nerve rootlets of lower-lumbar & sacral regions extend further down vertebral canal
- Filum terminale
- Connective tissue anchors cauda equina to the base of vertebral canal


Internal structure
- Grey matter
- All neuronal cell bodies
- 2 dorsal horns
- Nerve cells that receive sensory information from body via the dorsal root fibers
- 2 ventral horns
- Contain motor nerve cells
- Cell axons leave through ventral root fibers
- Lateral horns
- Present in thoracic & upper lumbar regions
- Autonomic motor nerves from sympathetic nervous system
- Exit spinal cord through the ventral roots
- White matter
- Ascending and descending fiber tracts
External structure
- Spinal nerves
- Merging of dorsal & ventral root fibers
- Carry mixed sensory and motor info to relevant body area
- Branches of spinal nerves
- Ventral rami – ventral branch
- Dorsal rami – dorsal branch
- Sympathetic chain
- Sympathetic ganglia
Information pathways: central → peripheral
Somatic
Afferent (sensory information)
- Receptor cells in periphery
- Info conveyed along peripheral axon → Soma (in dorsal root ganglion)
- Info conveyed along proximal axon → spinal cord (CNS)
- Info → ascending fibers (white matter) → brain for processing
Efferent (skeletal muscle)
- Neuronal cell bodies in ventral horn of grey matter
- Cell axon leaves spinal cord through ventral root → spinal nerve
- Axon flows out of ventral rami
- Directly innervates muscle at neuromuscular junction
Visceral
Afferent (sensory information)
- Receptors in viscera
- Info conveyed along peripheral axon → Soma (in dorsal root ganglion)
- Info conveyed along proximal axon → spinal cord (CNS)
- Info → ascending fibers (white matter) → brain for processing
Efferent (smooth muscle)
- Neuronal cell bodies in lateral horn of grey matter
- Cell axon leaves spinal cord through ventral root → spinal nerve
- Axon flows out of ventral rami
- Axon synapses with peripheral ganglia
- Peripheral ganglia innervates internal viscera
- Smooth muscle/glandular tissue/cardiac muscle
Neuronal Physiology
What is neurotransmission?
- Neuron → neuron/cell/organ/muscle/etc. Communication
- Point of communication → the synapse
Terminology
| Presynaptic neuron | The sender neuron |
| Synaptic cleft | Gap between cells |
| Postsynaptic cell | Receiver cell |
| Synaptic potential | Drive for transmission that mobilizes the synaptic vesicles to presynaptic membrane |
Neuron-neuron neurotransmission
Note: Neurons synapse with each other in 3 ways
Three types of synapses
- Axo-somatic
- Axon → cell body
- For modulatory effects
- Axo-axonic
- Axon → axon
- For all/nothing signals
- Axo-dendritic
- Axon → dendrite
- For multiple inputs to a neuron

Key ions in neurotransmission
| Na+ | Influx | To depolarize membrane to initiate/propagate an action potential |
| K+ | Efflux | To repolarize the membrane to resting potential once action potential has passed |
| Ca2+ | Influx | To trigger exocytosis of neurotransmitter into synaptic cleft |
Neuronal action potentials
- Resting potential: all voltage-gated channels closed
- At threshold, Na+ activation gate opens and [Na+] rises
- Na+ enters cell, causing explosive depolarization to +30 mV, which generates rising phase of action potential
- At peak of action potential, Na+ inactivation gate closes and [Na+] falls, ending net movement of Na+ into cell. At the same time, K+ activation gate opens and [K+] rises
- K+ leaves cell, causing its repolarization to resting potential, which generates falling phase of action potential
- On return to resting potential, Na+ activation gate closes and inactivation gate opens, resetting channel to respond to another depolarizing triggering event
- Further outward movement of K+ through still-open K+ channel briefly hyperpolarizes membrane, which generates after hyperpolarization
- K+ activation gate closes, and membrane returns to resting potential

Refractory periods during action potential
- Basically, the total time between a stimulus creating an action potential and the MP returning to rest.
- Determines how soon a neuron can respond to another stimulus.
- Divided into 2 sub-periods:
- Absolute Refractory Period – no additional stimulus (no matter how large) can initiate a further action potential.
- Relative Refractory Period – If an additional stimulus is to initiate another action potential during this time, it must be larger in order to reach threshold.
Two factors that influence the speed of an action potential
- Axon diameter → larger = quicker
- Presence of myelin (white matter) → impulse jumps from exposed axon-region to the next instead of having to open and close ion channels across the axon’s entire length (which would be slow)
Phases of neurotransmission
- Action potential reaches axon terminal, opens voltage-gated Ca+ channels
- Influx of Ca+ into axon terminal causes vesicles of neurotransmitter to migrate to the axon terminal.
- ‘Neurotransmitter’ released by exocytosis from the sending (pre-synaptic) neuron.
- Neurotransmitter (acetylcholine/noradrenaline/dopamine/glutamate/gaba/etc) diffuses across synaptic cleft between 2 neurons.

- Neurotransmitters bind to ligand-gated ion channels, causing change in membrane potential of postsynaptic neuron (dendrite) → creating graded potentials
- Graded Potentials can either Excite, or Inhibit the postsynaptic Neuron.
- If GP depolarizes membrane, it is excitatory
- If GP hyperpolarizes membrane, it is inhibitory

- Sum of graded potentials may cause membrane potential to reach threshold, triggering action potential. Neurotransmitter Inactivation by enzymes (e.g., ACh-Esterase) or reabsorption prevents continued stimulation.
Two types of postsynaptic receptors
Ionotropic (ligand-gated ion channels)
Mechanism: Binding of neurotransmitter → opening of ion channel → excitation/inhibition of cell
- Excitatory: Na+/Ca+ channel – opening → Na+/Ca++ Influx → Depolarisation of Membrane → “Excitatory Postsynaptic Potential” (EPSP)
- Inhibitory: Cl– Channel – opening → Cl– Influx → Hyperpolarization of membrane → K+ Channel – opening → K+ Efflux → Hyperpolarization of Membrane → “Inhibitory Postsynaptic Potential” (IPSP)
Metabotropic (G-protein linked receptors)
Mechanism: Binding of neurotransmitter → Activates G-protein → activates ‘effector’ proteins → activate secondary messengers (e.g., cAMP) → Regulates ion channels/activates enzymes/alters metabolism
| Ionotropic Receptors | Metabotropic Receptors |
 |
|
Actions of neurotransmission
- Direct physiological action
- e.g., Neuromuscular junction → muscle contraction
- e.g., Sympathetic synapse at SA node → ↑HR
- Links in a chain
- e.g., Peripheral sensory neuron → spinal cord → ascending sensory pathways → thalamus → cortex
- Modulation
- i.e., exerting a positive/negative influence on transmission by another neuron
Neurotransmitters
For a chemical to be a neurotransmitter, it must have
Dedicated synthesis
- Amine & amino-acid neurotransmitters are synthesized in the axon-terminal, however, peptide neurotransmitters are synthesized in the cell body & transported to the axon terminal.
- (This is because peptide synthesis requires gene transcription & translation which require a nucleus & rough endoplasmic reticulum.)
- There is a rate-limiting step for all neurotransmitter synthesis.
- (e.g., Activity/amount of an enzyme, substrate availability)
Active packaging
- Amine & amino-acid nt’s actively packaged into vesicles, driven by H+ gradient within vesicle. (i.e., H+-filled vesicles exchange H+ for neurotransmitter)
- Peptide NT’s packaged by Golgi apparatus & transported to axon terminal
Controlled release
- Various proteins involved in vesicle mobilization are activated by Ca++ influx (Note: Many such proteins are destroyed by botox, giving botox recipients expressionless faces)
- Vesicle-membrane fuses with presynaptic-membrane, creating a release-pore → NT diffuses across synaptic-cleft. often some NT’s end up in other neighboring synapses
Receptive post-synaptic cell
- Neurotransmitter activates either
- Ionotropic receptors (ligand-gated ion channels)
- Metabotropic receptors (G-protein linked receptors → secondary messengers)
Signal termination mechanism
- To prevent over-release of NT, autoreceptors exist on presynaptic membrane
- Provide negative feedback by inactivating adenylate cyclase → ↓cAMP → closes Ca++ channels → stop vesicle mobilization and release
- To prevent on-going stimulation, a NT’s signal is terminated by either
- Synaptic enzyme (destroy NT in synapse)
- Rapid re-uptake (note: for NT’s taken bac up, there are 2 fates)
- Recycling (repacked into synaptic vesicles)
- Enzymatic degradation (NT is broken down into metabolites)

http://what-when-how.com/neuroscience/neurotransmitters-the-neuron-part-1/
Regulation of receptor response
- If NT is over-released and/or not terminated → on-going stimulation → receptor activity is altered
- Desensitization
- ↓response to NT due to ↓sensitivity of receptor
- Down-regulation
- ↓response to NT due to ↓# of receptors
- Note: This functions to block out ‘noise’
- Desensitization
- If NT is under-released or if antagonist is administered for too long → receptor activity is altered
- Supersensitization
- ↑response to NT due to ↑sensitivity of receptor
- Up-regulation
- ↑response to NT due to ↑# of receptors
- Supersensitization
Neuromodulation
i.e., the fine-tuning (‘volume control’) of a signal
- A neuromodulator can be conceptualized as a neurotransmitter that is not reabsorbed by the presynaptic neuron or broken down into a metabolite. such neuromodulators end up spending a significant amount of time in the CSF (cerebrospinal fluid), influencing (or modulating) the overall activity level of the brain.
- Hence creates a broad signal across the brain → synchronous activation of separate regions → elicits markedly different level of responses from synaptic activity.
- Neuromodulators may either be released into a synaptic cleft, or extracellular fluid.
Types of neuromodulators
Some examples
- Metabolic products (e.g., adenosine, ATP, H+)
- Hormones (e.g., estrogen)
- Gases (e.g., nitric oxide, CO2)
- Amines (e.g., dopamine, serotonin, histamine, acetylcholine)
- Proteins
- Prostaglandins
The major neurotransmitters (classified by structure)
Amines (“classical neurotransmitters”)
- Acetylcholine (ACh)
- Dopamine
- Noradrenaline/norepinephrine (NA/NE)
- Serotonin/5-Hydroxyl tryptamine (5-HT)
Amino acids
- Glutamate (#1 excitatory neurotransmitter of the brain)
- GABA (𝝲-amino Butyric acid) (#1 inhibitory neurotransmitter of the brain)
- Glycine
Peptides
- Cholecystokinin
- Encephalins (e.g., endorphins, opioids) → turn off nociceptive/pain pathways
- Neuropeptide Y → regulates food intake/hunger
- Somatostatin
- TRH
- Vasoactive intestinal peptide (VIP)
Acetylcholine/ACh (cholinergic nerves)
Roles
- Brain functions
- Voluntary motor control
- Memory & learning pathways
- Arousal
- Sleep/wake cycles
- Peripheral functions
- Contraction of skeletal muscle
- Parasympathetic activity in the heart/GI/eye/salivary glands/lacrimal (tear) glands

Acetylcholine synthesis
- Choline + Acetyl CoA are combined by choline-acetyl-transferase (CAT) to form acetylcholine + CoA
- Hence, choline & acetate group from the acetyl-CoA combine → ACh
- Note: This occurs in the cytosol of the neuron at the axon terminal
Acetylcholine packaging
ACh is concentrated into vesicles by an ACh-transporter
Acetylcholine release
Via Ca++ mediated vesicular exocytosis
Cholinergic receptors (2 types)
- Muscarinic
- G-protein linked/metabotropic receptors
- Parasympathetic NS
- Nicotinic
- Ligand-gated ion channels/ionotropic receptors
- Neuromuscular junction/CNS/PNS
ACh signal-termination
- ACh is degraded within the synapse by acetyl-choline esterase → choline + acetate
- The choline released is actively transported back into the presynaptic cell by a choline transporter
Rate-limiting step
- The reuptake of choline, because the availability of choline determines the amount of ACh synthesis
Catecholamines [dopamine/NE(NA)/epinephrine (adrenaline)]
Dopamine
Roles
- Brain functions
- Voluntary motor control
- Cognition
- Reward center
- Emotions and behavior
- Vomiting
- Peripheral functions
- Cardiovascular function (↑HR & contraction)
- Renal vasodilation at JG apparatus (↑filtration)
Synthesis
- Starts with tyrosine (amino acid)
- Tyrosine is converted to dopa by tyrosine-hydroxylase
- Dopa is converted to dopamine by dopa-decarboxylase
Packaging
- Dopamine is packaged into vesicles in axon terminal
Release
- Via Ca++ mediated vesicular exocytosis
Dopaminergic receptors
- Are metabotropic (G-protein linked receptors)
- Note: All catecholamine receptors are metabotropic
Dopamine signal-termination
- Active reuptake into the axon via Na+-dependent transporters → repackaged/destroyed
- Note: If destroyed via enzymatic degradation by mono-amine oxidase (MAO)
Rate-limiting step
- Conversion of tyrosine → dopa by tyrosine-hydroxylase
- Hence, the activity of tyrosine-hydroxylase is rate-limiting for all catecholamine synthesis


Norepinephrine
Roles
- Brain functions
- Attention/arousal (fight/flight response)
- Sleep-wake cycle
- Learning & memory
- Anxiety
- Pain
- Mood
- Peripheral functions
- Sympathetic responses
- ↑HR + BP
- ↑Glycolysis + gluconeogenesis + fat metabolism
- ↑Blood flow to muscles
- ↑Blood flow to coronary circulation
Synthesis
- Starts with tyrosine (amino acid)
- Tyrosine is converted to dopa by tyrosine-hydroxylase
- Dopa is converted to dopamine by dopa-decarboxylase
- Dopamine is packaged into vesicles in axon terminal
- Dopamine is converted to norepinephrine (NA) by dopamine-hydroxylase inside the vesicles
Packaging
Via Ca++ mediated vesicular exocytosis
Adrenergic receptors
Are metabotropic (G-protein linked receptors)
Note: All catecholamine receptors are metabotropic
Signal-termination
Active reuptake into the axon via Na+-dependent transporters → repackaged/destroyed
Note: If destroyed, via enzymatic degradation by mono-amine oxidase (MAO)
Rate-limiting step
- Conversion of tyrosine → dopa by tyrosine hydroxylase
- Hence, the activity of tyrosine-hydroxylase is rate-limiting for all catecholamine synthesis

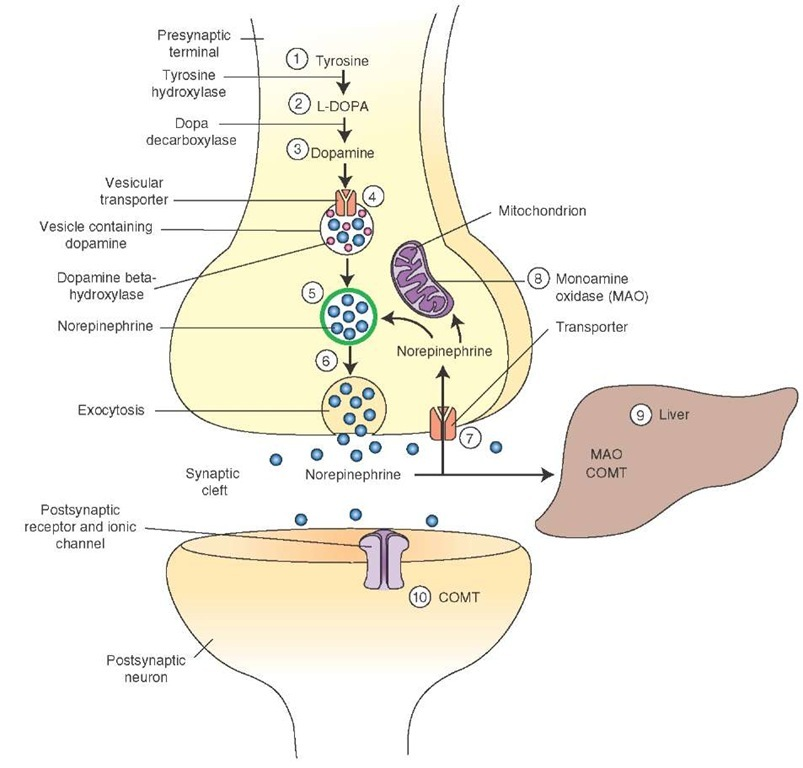
http://what-when-how.com/wp-content/uploads/2012/04/tmp1474_thumb1.jpg
Serotonin
Roles
- Brain functions
- Pain
- Wakefulness/arousal
- Sleep-wake cycle
- Mood and emotions
- Vomiting
- Circadian rhythm (indirectly by conversion to melatonin)
- Peripheral functions
- GI tract
- Platelet function
Synthesis
- Starts with tryptophan
- Tryptophan is converted to 5-HTP by tryptophan hydroxylase
- 5-HTP is converted to 5-HT (serotonin) by 5-HTP-decarboxylase
Packaging
Serotonin is packaged into vesicles in axon terminal
Release
Via Ca++ mediated vesicular exocytosis
Serotonergic (5-HT) receptors
“5-HT” receptors (can have ionotropic & metabotropic types)
Signal-termination
Active reuptake into the axon via Na+-dependent transporters → repackaged/destroyed
Note: If destroyed, via enzymatic degradation by mono-amine oxidase (MAO)
Rate-limiting step
- Availability of tryptophan in the extracellular fluid (tryptophan is an essential amino acid)
- Hence, a dietary deficiency of tryptophan → depletion of serotonin in the brain


Amino acid neurotransmitters
Glutamate
Roles
Most common neurotransmitter in the brain
Synthesis
- Begins with conversion of glucose → ɑ-Ketoglutarate via glycolysis and TCA cycle
- Then conversion of ɑ-Ketoglutarate → glutamate via a transaminase reaction
Packaging
Active packaging in vesicles
Release
Ca++ dependent exocytosis
Receptors
- Ionotropic
- NMDA receptor
- Kainate receptor
- AMPA receptor
- Metabotropic
- mGluR receptor
Signal-termination
K+ dependent reuptake into presynaptic neuron → repackaged into vesicles

GABA (Gamma Amino Butyric Acid)
Roles
Inhibitory neurotransmitter in brain
Synthesis
- Begins with conversion of glucose → ɑ-Ketoglutarate via glycolysis and TCA cycle
- Then conversion of ɑ-Ketoglutarate → glutamate via a transaminase reaction
- Then conversion of glutamate → GABA by glutamic-acid-decarboxylase (+VitB6)
Packaging
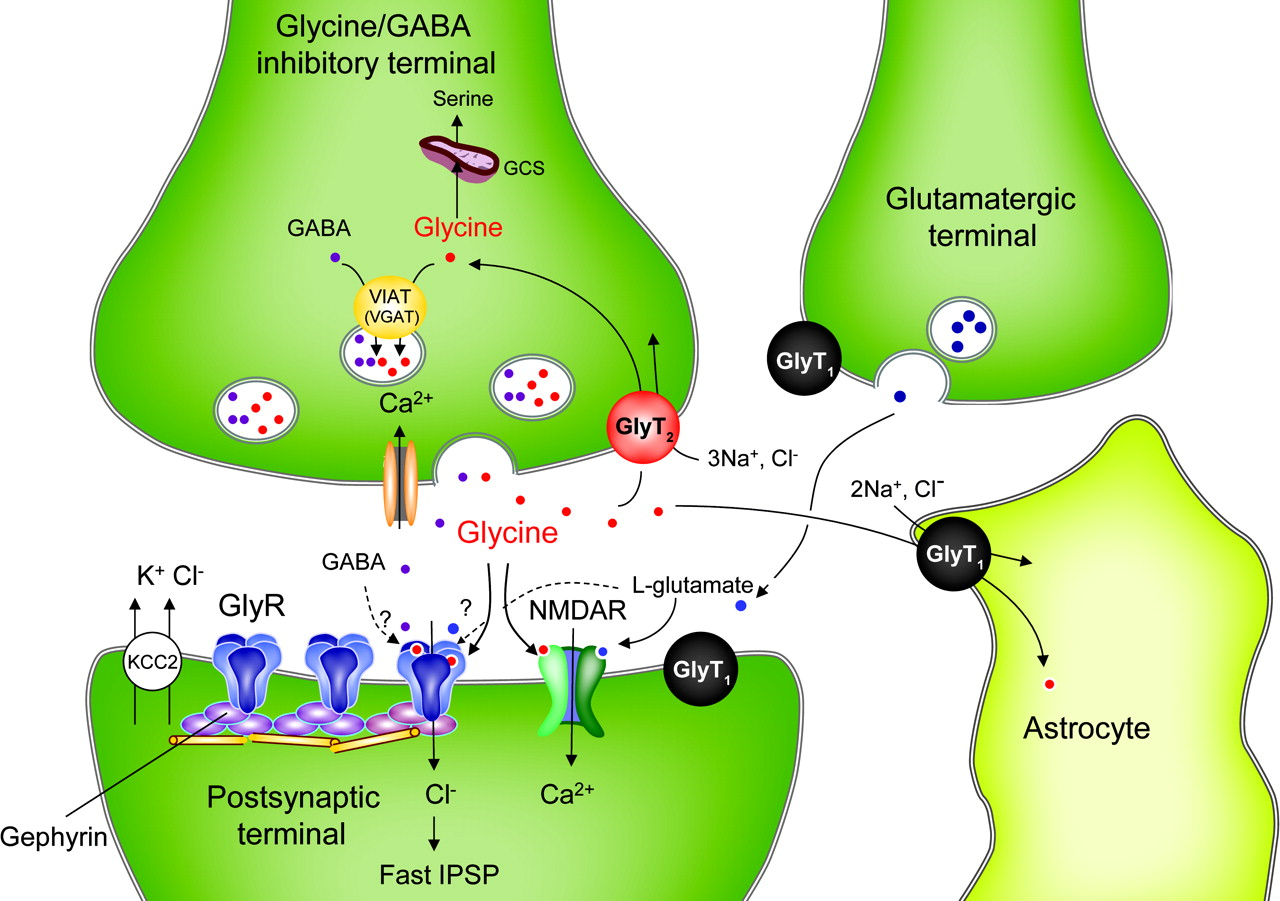
Packaged into vesicles by the vesicular GABA transporter (VGAT)
Release
Ca++ dependent exocytosis
Receptors
- GABAA → ligand-gated Cl– channels (ionotropic) stimulation → Cl– influx → hyperpolarizes
- GABAB → G-protein linked (metabotropic) stimulation → K+ efflux → hyperpolarizes
Signal-termination
K+ dependent reuptake into presynaptic neuron → destruction by GABA-transaminase

Glycine
Roles
- Inhibitory NT in the forebrain, brainstem, spinal cord
- Motor functions
- Sensory functions
Synthesis
Begins with glucose → 3-phospho glycerate → serine → glycine
Packaging
Vesicles
Release
Ca++ dependent release
Receptors
Ionotropic Cl– receptors → Cl– influx → hyperpolarization
Signal-termination
Reuptake of glycine into presynaptic neuron
Neurobiology of Memories
Process of memory creation
External stimuli
Sensory input bombards the brain, and is sent to the cerebral cortex
Temporary storage (cerebral cortex)
- Sorts and evaluates the information
- Depending which inputs you focus on, determines what info is sent to short term memory
- Input not focused on is forgotten
Short term memory
- In medial temporal lobe (hippocampus, amygdala, surrounding cortical areas)
- Excitement/rehearsal/association/emotion → transfer to long term memory
- Input not subjected to the above is forgotten
Long term memory
- Requires ACh → for declarative; or dopamine → for non-declarative
- Declarative: stored in prefrontal cortex
- Non-declarative: stored in premotor cortex

Short term memory (STM)
- Based in hippocampus
- However, small links are established with cortex (visual/auditory/olfactory/gustatory)
- These links are made by changes to neuron signaling that don’t require protein synthesis (quicker)
- Last seconds → several hours maximum (aka: “crammers” memory)
- i.e., changes to neurons are transient (temporary)
- Limited to ~7-8 “chunks” of information
- Amnesia = damage to connection between STM & LTM
Working memory
- Note: Often grouped with STM
- Temporary retention, integration (with other brain areas), manipulation of sensory information to facilitate a response
- e.g., crossing the road
- Look left (remember position of cars)
- Look right
- Look left again (compared position of cars to the initial look → is it safe to cross?)
- Associated with prefrontal cortex
- Closely tied to STM
- Neurotransmitter
- Dopamine

Long term memory (LTM)
- Based in hippocampus
- Limitless capacity → the amount we can remember depends on access rather than capacity
- Usually requires STM input
- Generally LTM-creation requires the info to pas through STM first
- However, some information can bypass STM by ‘hijacking’ existing LTM links (e.g., typing a fact to a previously-learned fact)
- LTM creation – influenced by 4 factors
- Genetics
- Age
- Trauma
- Malnutrition
- LTM creation – improved by
- Positive/powerful emotional state
- Rehearsal
- Association of new data with old data
- The belief that memory is important
- Requires remodeling the neuron/synapse via long term potentiation and long term depression
Long term potentiation (LTP)
- Definition: “A long-lasting postsynaptic depolarisation, induced through repetitive stimulation & summation of excitatory postsynaptic potentials.”
- Simply: a persistent increase in synaptic strength
- Calcium
- #1 mediator of LTP
- NMDA-mediated Ca++ influx → activation of enzymes that cause
- ↑NT release
- Or changes in postsynaptic receptors
- The #1 NT: glutamate → binds to NMDA and/or AMPA receptors
- NMDA receptors
- Act as coincidence detectors (simultaneous signals)
- i.e., detects coupling of occurrences
- Is essentially a ligand (glutamate)-gated Ca++ channel
- Has a voltage-dependent Mg+-block → acts as a voltage gate
- Therefore, NMDA receptor is ligand and voltage-gated
- AMPA receptors
- Is a ligand-gated Na+ channel
- When glutamate binds → channel opens → depolarization → AP
- AP kicks out of the Mg+ block on the NMDA receptor
- NMDA receptors
- 3 Phases of LTP
- Induction (synaptic plasticity)
- Alleviating of the NMDA receptor’s Mg+ block
- This may be done by
- AMPA-receptor mediated AP
- Metabotropic-receptor linked to ion channel → AP
- This may be done by
- Alleviating of the NMDA receptor’s Mg+ block
- Expression (synaptic augmentation)
- Modify proteins in postsynaptic terminal or ↑in presynaptic neurotransmitter release → strengthens response to subsequent stimuli
- Activation of genes in postsynaptic neuron’s nucleus → synthesis of synaptic proteins → ↑synaptic strength
- Maintenance (long term loss/continuation of LTP)
- Rise in mRNA levels → augmented synthesis of proteins linked to memory
- This ↑in protein synthesis is regulated by a (+)transcription factor: “cAMP response element binding” protein (CREB).
- This perpetual ↑protein-synthesis → long-lasting ↑synaptic strength that is believed to underlie memory.
- Rise in mRNA levels → augmented synthesis of proteins linked to memory
- Induction (synaptic plasticity)

Long term depression (LTD)
- Definition: The weakening of a neuronal synapse that lasts from hours-days
- Calcium, the #1 mediator of LTP
- NMDA-mediated Ca++ influx → activation of phosphatases that cause
- De-phosphorylation of AMPA-receptors
- → in hippocampus → AMPA dephosphorylation → ↓amplitude of postsynaptic potential to the normal level (prior to LTP)
- → can also remove receptors from post-synaptic membrane & place them in reserve
- De-phosphorylation of AMPA-receptors
- NMDA-mediated Ca++ influx → activation of phosphatases that cause
- Results from
- Strong synaptic stimulation (cerebellum) or
- Persistent weak synaptic stimulation (hippocampus)
- Function in
- Overall
- Plays a role in modulating impact of formed memories to prevent overload
- Hippocampus
- Thought to return LTP’d synapses back to a normal level so they will be available to store new information
- Cerebellum
- Thought to promote motor learning
- Overall
2 types of long term memory
Declarative (explicit)
- Brain regions
- Hippocampus
- Para-hippocampal regions (medial temporal lobe)
- Areas of cerebral cortex
- Thalamus + hypothalamus
- Learning “WHAT”
- Facts/words/ideas/concepts/events

Non-declarative (implicit)
- Learning “HOW” – how to do things/how to recognize things
- Procedural
- Walking
- Driving a car
- Doing algebra
- How to get home
- Priming (anticipation) – i.e., the use of a trigger to pull out a memory
- Ache in gut if you get a letter from tax office – due to previous association
- Reaction to seeing your partner
- Classically-conditioned
- Emotional
- e.g., fear when seeing a shark
- e.g., ringing bell → dog salivates
- Motor
- Emotional
- Non-associative
- Isolated events not linked to anything
- Procedural

Circuit of declarative memory
- Outside stimuli
- Afferent sensory information → sensory nerves → spinal cord → medulla → brain (somatosensory cortex)
- Somato-sensory cortex
- Sensory information is sorted and evaluated
- Whatever is the main focus of your attention is prioritized → sent to STM in medial temporal lobe (hippocampus, amygdala, surrounding cortical areas)
- Medial temporal lobe areas
- Role: memory consolidation and retrieval via communication with thalamus & prefrontal cortex
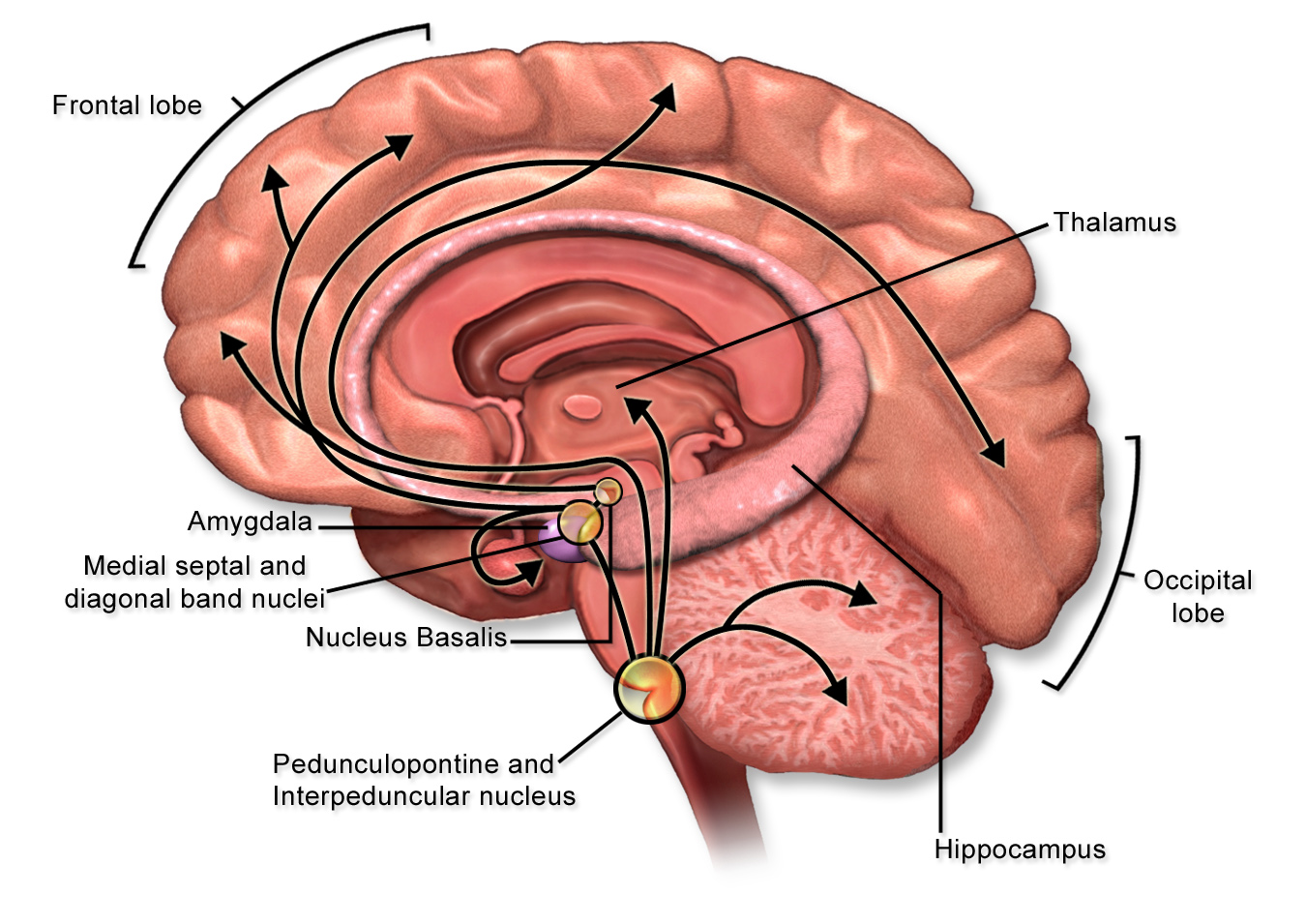
- Basal forebrain
- Primes the medial-temporal lobe and prefrontal cortex with ACh → triggers LTP in hippocampus
- Enables LTM formation (loss of ACh in Alzheimer’s ↓Memory formation & retrieval)
- Feedback to association cortices
- Facilitates retrieval of memories

Circuit of non-declarative (procedural) memory
- Sensory & motor input
- Afferent sensori-motor information → spinal cord → medulla → brain (association cortices)
- Association cortices
- Somatosensory/visual/auditory/etc.
- Relay sensori-motor inputs to the basal nuclei
- Basal nuclei
- Relays sensori-motor inputs through the thalamus to the premotor cortex
- Substantia-nigra
- Releases dopamine onto basal nuclei → prime this circuit (note: loss of dopamine input: i.e., Parkinson’s → interferes with procedural memory)
- Premotor cortex
- Plans and organizes learned actions

Common memory disorders
Alzheimer’s
- What?
- Progressive memory loss (“mild cognitive impairment”), dementia, overwhelming retrograde & anterograde amnesia
- No real diagnostic tests
- Genetic etiology (autosomal dominant)
- Amyloid precursor-protein gene
- Presenilin 1 gene
- Presenilin 2 gene
- Symptoms due to
- Loss of ACh innervation onto prefrontal cortex & medial-temporal lobe (hippocampus) by basal forebrain
- Affects
- Basal forebrain cholinergic system (i.e., loss of ACh innervation)
- Striatum (caudate & putamen) → part of basal ganglia
- Thalamus
- Cerebellum
- Inability to
- Define simple words
- Understand use of common items
- Comprehend numbers
- i.e., loss in declarative memory
- Emotional disturbances
- Confusion
- Agitation
- Delusion
- Paranoia
Amnesia
- Typically declarative memory loss (therefore hippocampal damage)
- Commonly caused by temporal lobe damage (hippocampus and/or thalamus)
- L-hippocampus = language
- R-hippocampus = spatial memory
- Anterograde
- Inability to form new memories from time of injury/damage onwards
- Non-declarative memory is unaffected
- Retrograde
- Inability to recall memories from time of injury/damage backwards
Korsakoff
- Anterograde & retrograde amnesia
- Caused by severe thiamine deficiency (alcoholics & severe malnutrition)
- → loss of connection between temporal lobes (hippocampus) and frontal cortex
Seven ‘sins of memory’ – types of memory deficits
- Transience – memory ‘fade’
- Absent-mindedness – brushing teeth when already brushed them
- Blocking – when a memory is on the ‘tip of the tongue’
- Misattribution – where you misremember where you saw/heard something, or even if
- Suggestibility – where someone suggests that you saw/heard something (when you didn’t) and you ‘remember’ seeing/hearing it
- Bias (negative bias) – tend to recall only the negative things
- Persistence – remember a single failure rather than multiple successes (e.g., post exam briefings)
- … Confabulation – when you elaborate on a memory
Neurobiology of Emotions
Definitions
| Affect | Experience of a feeling/emotion that’s not related to bodily changes |
| Emotion | A mental and physiological reaction to stimuli, experienced as affect plus physiological changes in the body |
| Feelings | A partly mental, partly physical response to a person, thing, or situation, marked by pleasure, pain, attraction, or repulsion |
| Arousal | The visceral (body’s) response to stimuli, including autonomic nervous system and neuro-endocrine activity |
| Cognition | The process of knowing, including both awareness and judgment |
| Behavior | The active response to stimuli (posture, facial expression, speed, eye movement, vocalization, etc.) |
Emotion
Why does it exist?
- Critical to survival
- Both the ability to experience emotion, and to recognize others’ emotions
- Gut reactions
- Recognizing danger, fried/foe
- Vital to decision making
- Important role in learning
Theories of emotion
- A link exists between physiological responses to stimuli & effect of emotion, but which comes first?
- Cannon-Bard Theory
- Conscious awareness of emotion comes first, then visceral reactions
- James-Lange Theory
- Visceral reactions come first, then the conscious emotional experience follows
- Cannon-Bard Theory

- Currently, the most plausible theory
- Visceral reaction (physiological responses) comes first, causing the emotional experience (feelings & thoughts)
- However, the emotional experience can influence and/or perpetuate the visceral response

3 phases/components/types of emotion
Primary emotions
- What is felt first → the first instantaneous emotion (usually the simplest/primitive emotions)
- General independent of culture (universal)
- Joy
- Sadness
- Anger
- Fear
- Surprise
Secondary emotions
- What is felt second → what the primary emotion leads to (slightly more complex emotion)
- Generally a combination of primary emotions + context
- Affection/love
- Lust
- Contentment
- Disgust
- Envy
- Guilt
Tertiary emotions
- An aggregate of primary and/or secondary emotions (the most complex emotions)
- Generally the result of a decision, taking into account many factors
- Satisfaction
- Hope
- Frustration
- Gloom
- Contempt
Physiological context of emotions
- The physiological state of a person and body can influence resulting emotions and emotional reactivity
- Well-being
- Depression
- Calm
- Tense
- Fatigue
Brain regions involved in recognition, induction, and regulation of emotions
Thalamus
- Funnels sensory information to amygdala, and the cerebral and cingulate cortices
- Important in fact-based (explicit) memory
Cingulate gyrus
- Regulates attention
- Emotional ‘coloring’
Ventromedial prefrontal cortex
Conscious recognition of emotions
Cerebral hemispheres
- R-brain → more associated with negative emotions
- L-brian → more associated with positive emotions
Sensory cortices & association areas
- Recognition of stimuli
- Sensory cortices: visual, auditory, olfactory, gustatory, tactile
- Sensory association areas: novel VS. familiar
Insula
Involved with recognition and feeling of disgust

The Papez circuit
- Thalamus relays sensory input to cingulate cortex
- Cingulate cortex gives you the emotional experience; it also relays to the neocortex, which gives context/coloring to the emotion; also relays to hippocampus
- Hippocampus relays to the hypothalamus, causes emotional expression (visceral response)

The limbic system
Amygdala
- #1 structure involved in emotion → the “heart” of the limbic system.
- “The fight/flight center”
- Linked to all but 8 areas of the cortex → thought to be #1 integrator of cognitive & emotional info
- Afferents (receives input from)
- Brainstem – inputs associated with physical states (BP/HR/etc)
- Hypothalamus – inputs associated with physical states (BP/HR/etc)
- Thalamus – sensory info
- Hippocampus – inputs associated with explicit memory
- cortex – sensory inputs & decisions related to perceived threats
- Efferents (sends output to)
- Brainstem – influences visceral fear-driven, fight/flight responses
- Hypothalamus – influence on memory & aggression
- Thalamus – influences processing of new sensory info
- Hippocampus – fear is an important driver for learning & memory
- Prefrontal cortex – fear is important in decision making & cognition
- Regulates
- Fear & aggression
- Vigilance & attention
- Recognition of emotion (in self & others)
- Emotional contribution to memory (emotional implicit memory)
Hypothalamus
- Visceral responses to emotion
- Aggression
- Sex drive
Brainstem
- Visceral responses to emotion

Neurotransmitters and emotion
Noradrenaline (a target for antidepressants)
- Activated by novel, unexpected stimuli
- Released by
- Locus coeruleus (a nucleus in the pons involved with physiological responses to stress and panic)
- Regulates
- Mood/arousal
- Anxiety
- Pain
- Sleep/wake cycles
- Motor activity
Serotonin (a target for antidepressants)
- Activated by general activity/arousal
- Released by raphe nuclei ( a group of nuclei in the brainstem)
- Regulates
- Mood
- Emotions
- Sleep/wake cycles
- Dominance/aggression
- Anxiety
Dopamine
- Activated by pleasurable activities
- Released by
- Ventral tegmental area (VTA)
- Substantia nigra
- Regulates
- Somehow plays a role in regulation of perception of emotion
- Involved in reward center
Glutamate & GABA
Reduces anxiety
Acetylcholine
- Released by basal & septal nuclei of Meynert
- Regulates
- Cognitive processing
- Arousal and attention
The emotion of fear
- Brain structures involved
- Thalamus → amygdala
- Thalamus
- → primary sensory cortex
- → association cortices
- Long and short pathways
- Long
- Info processed by higher brain centers and hippocampus
- Results in a more complex response
- Short
- Info sent straight to amygdala
- Results in a basic response (Recoil from stimulus/freeze)
- Advantage = no cortical processing means quicker reaction times = ↑survival
- Long
- Process of fear
- Sensory information enters brain → thalamus
- Thalamus sends information to amygdala (via long/short route)
- Amygdala activates visceral responses through hypothalamus
- Amygdala activates ventromedial prefrontal cortex (allows conscious recognition of the emotion)
- Visual cortex also informs prefrontal cortex about the threat

Aggression
- Affective aggression VS. predatory aggression
- Predatory aggression is related to feeding behavior and isn’t accompanied by sympathetic physiological response with which affective aggression is associated
- Associated structures
- Cerebral cortex
- Amygdala
- Hypothalamus
- Periaqueductal grey matter (PAG)
- Ventral tegmental area (VTA)
i.e., Aggression is controlled by a neural pathway from amygdala through hypothalamus, PAG, and VTA.
- Neurotransmitter: serotonin
- Possible hormonal link: adenosine
Pleasure and reward: the ‘reward circuit’
- Brain structures involved
- VTA
- Nucleus accumbens
- Amygdala
- Prefrontal cortex
- Thalamus
- Neurotransmitters involved
- Dopamine → VTA & nucleus accumbens

Somatosensory Processing
Sensation types
Note: Sensations are initiated by receptor activation
Tactile
- Touch
- Vibration
- Stretch
- Pressure
- Itches
Temperature
Hot/cold
Pain
Aka ‘nociception’
Visceral
- Blood pressure
- pH
- O2
- CO2
What are sensory receptors?
Specialized nerve endings that monitor and respond to the environment.
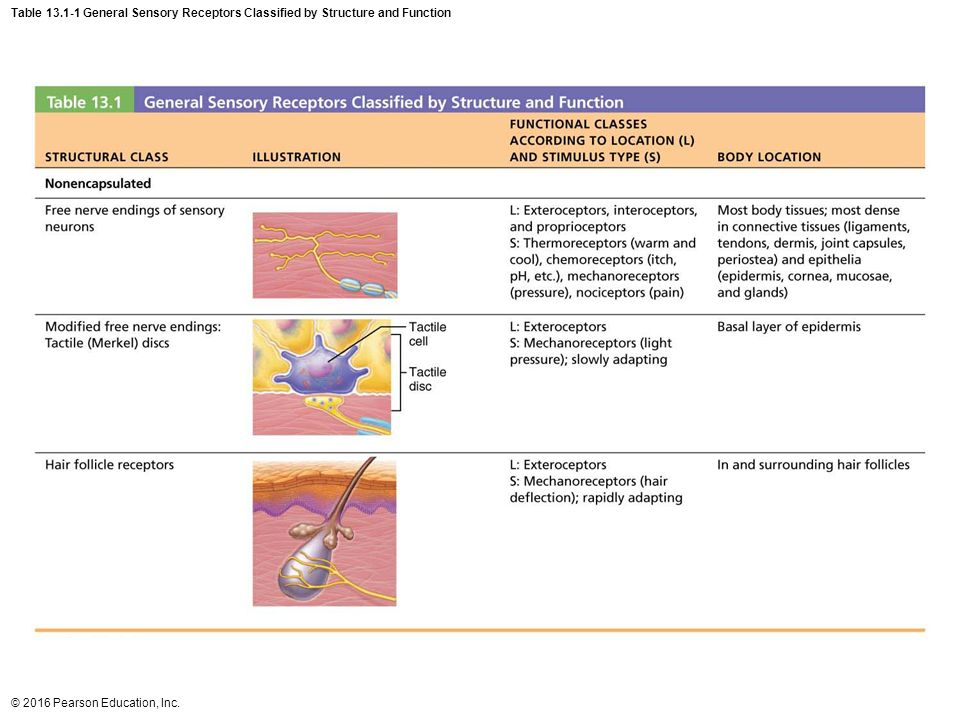
Classification of sensory receptors based on 3 things
Physical location
| Exteroceptors | Located in skin (respond to external stimuli) |
| Interoceptors | Located viscerally (respond to internal stimuli) |
| Proprioceptors | Located in muscle/bone/tendon |
Type of stimulus
| Mechanoreceptors | Respond to physical forces |
| Thermoreceptors | Respond to temperature |
| Nociceptors | Respond to damaging stimulus |
| Chemoreceptors | Respond to chemicals (smell/taste OR blood O2/CO2/H+) |
| Photoreceptors | Respond to light (eyes) |
Receptor structure
| Simple | Naked (“free”) nerve endings (pain & temperature) |
| Complex | Structurally elaborate nerve endings (pressure, vibration, stretch) (enhances specificity) |
Why are pain receptors ‘simple’?
Pain, a basic survival mechanism, would have been first to evolve and its receptors have been sufficient since. Hence there has been no need for pain receptors to evolve further.

Receptor transduction
- Receptors respond to stimuli by transduction them into electrical signals
- These electrical signals = ion movements across the membrane → changes in membrane potential
- These changes in membrane potential are graded (i.e., stimulatory/inhibitory, depolarization/hyperpolarization)
- These graded potentials at the receptor level = receptor potential

- Receptor potentials may summate to threshold → initiating an action potential
- These action potentials at the receptor level = general potentials

Receptors: nature of activity
When are they active?
- Tonic receptors: continually firing (e.g., proprioceptors)
- Phasic receptors: fire only with a change in the environment (e.g., thermoreceptors)
When do they inactivate? (How quickly do they adapt?)
Note: Adaptation = time taken for receptor to stop firing during sustained stimulation
- RARs – rapidly adapting receptors
- Receptor quickly stops firing under continuous stimulus
- e.g., touch receptors (can’t feel clothes after a while)
- SARs – slowly adapting receptors
- Receptor maintains firing under continuous stimulus
- e.g., muscle stretch receptors (proprioceptors)
Receptive fields
A receptive field: the area monitored by 1x receptor (i.e., touch anywhere in that field, the sensation will come from the entire receptive field)

- Large receptive fields
- Low receptor density
- Poor localization
- e.g., skin on your back

- Small receptive fields
- High receptor density
- Good localization
- e.g., skin on your fingertips
- Note: 2 point discrimination is best with small, dense receptor areas
Receptor types

Receptor speed
- Varies by diameter and myelination – affects speed of conduction and therefore type of sensory information
- Larger + myelinated = fastest
- Smaller + non-myelinated = slowest
- Proprioceptors are fast to ensure fine motor control
- There are 2 types of paint receptors: the fastest is responsible for initial (sharp) pain
- Slowest is responsible for dull ache that follows

Initial processing by thalamus
- Once sensory input enters CNS, it travels to the Thalamus (sorting station of the brain)
- Impulses are sorted on the basis of where they came from and the type of sensation
- They are then sent to their relative functional areas on the cortex (brain surface).
- Response: If a response is required, then a discrete area of the brain will activate it.
- Primary motor cortex: voluntary motor
- Language & Speech Centres: vocalization
- Hypothalamus & Brain Stem: visceral responses (chest/abdominal – pulse/sweat/BP)

Functional sensory areas of the brain
- Primary visual area – receives visual information from the retina of the eye.
- Primary motor area – controls voluntary skilled movements of our skeletal muscles
- Pre-motor cortex – controls learned motor skills (musical instruments/typing/etc)
- Primary auditory area – sound energy stimulates hearing receptors and is interpreted as pitch/vol/location
- Primary somatosensory area – receives information from the general (somatic) sensory receptors
- Primary gustatory area – perception of taste stimuli
- Primary Olfactory area – info from smell receptors

Somatosensory association area
- The somatosensory cortex has connections to the somatosensory association areas
- Gives meaning to the received information, store it in memory, relate it to past experiences & decide on plan of action
Somatosensory cortex
- Roles
- Detection of sensation & conscious awareness of sensation
- Feature/quality recognition (ie. texture/size/shape)
- Exhibits ‘somatotopy’ (body mapping)
- i.e., specific cortical areas responsible for particular body regions
- Receptor density in a body region determines the size of the respective cortical area

Somatosensory pathways
First order neurons (peripheral afferent nerves)
- e.g., dorsal root of spinal nerves and sensory cranial nerves
- Sensory information is frequency coded
- Enter spinal cord via dorsal nerve root → terminate in dorsal horn
- Note: Cell bodies of the pseudounipolar-neuron receptors culminate in the dorsal root ganglion
Second order neurons (ascending pathways of spinal cord)
- Once inside the spinal cord, 1st order neurons → synapse with 2nd order neurons
- 2nd order neurons
- Often responsible for decussation (crossing of fiber tracts to the other side of the body)
- Different sensory information takes different ascending pathways to the brain
Third order neurons
- Note: 3rd order neurons are only relevant to the dorsal column and the spinothalamic pathways
- Spinocerebellar pathway terminates in the cerebellum with 2nd order neurons
- Carry sensory information from thalamus to the primary somatosensory cortex in parietal lobe
- Thalamus sorts incoming sensory information → sends it to the cortex

The 3 ascending pathways
Dorsal column pathway
- Synapses with 2nd-order neurons in medulla
- Decussate in the medulla
- Neurons are
- Large & myelinated
- Rapidly adapting
- Sensory info
- Touch
- Vibration
- 2-point discrimination
- Proprioception

Spinothalamic pathway
- Synapses with 2nd-order neurons in spinal cord at level of spinal root
- Decussate in spinal cord at level of spinal root
- Neurons are
- Small & myelinated
- Slowly adapting
- Sensory info
- Crude touch & pressure
- Pain
- Temperature

Spinocerebellar pathway
- Synapse with 2nd-order neurons in spinal cord
- Doesn’t decussate – remains ipsilateral
- (“On the same side of the body”)
- Neurons are
- Large & myelinated
- Slowly adapting
- Sensory info
- Proprioception from
- Muscle spindles
- Golgi tendon organs
- Joint capsules
- → coordinate skeletal muscle activity
- Proprioception from

Neurotransmitters (NTs) and receptors
At the sensory nerve
- TRPV1-Receptor (Ca++ Channel)(“TRP Vanilloid Receptor1”). Opened by:
- Capsaicin (from hot chillies)
- Heat
- Mechanical (Mechanism unclear)
- H+ (Acid) (often a result of inflammation)
- Bradykinin receptors
- Bradykinin receptor activates TRPV1-Receptor → Depolarization → Nociception
- Prostanoid receptors
- Sensitive to prostaglandins
- Open Na+ channels →*
- Inhibit K+ channels →*
- Open TRPV1-receptors →*
*→ ↑MP → Lowers threshold → ↑sensitivity
- ASIC – (“acid sensitive (gated) ion channel”)
- Acid → ASIC-stimulation → depolarisation of cell → nociception
- Opiate/cannabinoid receptors
- Sensitive to opioid & cannabinoids
- Open K+ channels → K+-efflux → ↓MP (hyperpolarizes cell) → ↓sensitivity

At the dorsal horn
- Afferent pathway
- Substance P
- Glutamate (AMPA & NMDA receptors)
- Efferent pathway – sensory modulation via pain-gate mechanism
- Opioids activate descending inhibitory pathways & directly inhibit dorsal horn synapse
- Noradrenaline directly inhibits dorsal-horn synapse
- Serotonin (5-HT) directly inhibits dorsal-horn synapse
- Encephalins directly inhibit dorsal-horn synapse
- Note: Low-dose tricyclic antidepressants can treat neuropathic pain by blocking reuptake of NE, 5-HT, & encephalins in dorsal horn synapse
Motor Processing
Hierarchy of structures – the levels of motor control
- Ready (strategy) – deciding “what to do”
- Prefrontal cortex
- Somatosensory association cortex (area 5)
- Basal ganglia (Note: Basal ganglia are the interface between strategy and tactics)
- Set (tactics) – deciding “how to do it”
- Basal ganglia
- Pre–motor area (PMA)
- Supplementary motor area (SMA)
- Go (execution) – “action”
- Primary motor cortex (M1)
- Cerebellum
- Brainstem
- Descending tracts
- Spinal nerves
- Peripheral motor neurons
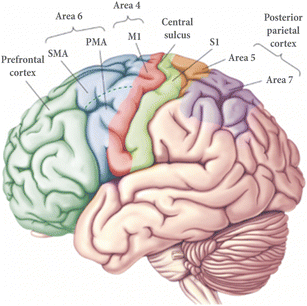
Roles of these brain regions (in motor processing)
Prefrontal cortex
Consciously decides “what movement” is required for the desired outcome (managerial function)
Somatosensory association areas
Tells the brain where the body is in space (proprioception)
Premotor area & supplementary motor areas
- Plans “how to do the movement”
- Is also the memory bank of complex, patterned, and highly skilled learned movements
Primary motor cortex (M1)
- “Initiates the movement” (typically precise or skilled voluntary movement)
- Note: M1 also exhibits somatotopy – the bigger the cortical area, the more precise the movements
- Receives direct and indirect inputs
- Direct → from: prefrontal cortex, SMA/PMA, somatosensory areas
- Indirect → from: cerebellum (via thalamus)
- Broca’s area controls the muscles responsible for speech (tongue/jaw/lips/face)

Basal ganglia
- Involved in action-selection and initiation of voluntary & patterned movements (e.g., walking)
- Motor control
- Motor learning
- Note: also has a role in cognition & memory
- A loop exists between cortex → basal ganglia → thalamus → premotor cortex → cortex
- Receives inputs from the entire cortex
- SMA/prefrontal cortex/sensory cortex/M1
- Information travels through basal ganglia in this order: striatum → globus pallidus
- Sends information to the PMA & SMA via the ventro-lateral nucleus of the thalamus (VLo)
- Receives inputs from the entire cortex
- Consists of
- Striatum
- Caudate nucleus (cognition + behavior)
- Putamen (motor) → automatic performance of previously learned movements
- Globus pallidus
- Striatum
- Other associated structures
- Subthalamic nuclei
- Substantia nigra (eye movement + motor planning, reward seeking, learning, addiction)

http://brainmind.com/GlobusPallidus.html

Note: The globus pallidus is spontaneously active!
Globus pallidus → thalamus (inhibits thalamic-SMA activity → keeps the SMA “quiet”)

Cerebellum
- Functions
- Precise timing & appropriate patterns of skeletal muscle contraction – required for smooth, coordinated movements & agility needed for daily living (driving/typing/playing music/etc.)
- Involved in the correct sequencing & coordination of muscle contractions
- Involved in motor learning – compares intention with result & corrects for next time
- Balance & posture
- Note: Cerebellar activity is subconscious (i.e., we have no awareness of its functioning)
- A loop exists between the cortex → pons → cerebellum → thalamus → M1 → cortex
- Receives inputs from the cerebral cortex (M1, pma, *somatosensory areas) via the pons
- Also receives proprioceptive feedback
- Sends info to the primary motor cortex (M1) via the ventrolateral nucleus of the thalamus
- Informs primary motor cortex (M1) about direction, force, & timing of movements
- Receives inputs from the cerebral cortex (M1, pma, *somatosensory areas) via the pons
- Output into descending pathways:
- Vermis → ventromedial pathways
- Hemispheres → lateral pathways
- Cerebellar processing
- Cortical motor areas notify the cerebellum (via ‘relay nuclei’ in the brainstem) of their intent to initiate voluntary muscle contractions.
- Constant proprioceptive input (muscle/tendon tension, joint position, etc.) enables the cerebellum to evaluate the body’s position & momentum.
- Cerebellum calculates optimum force, direction, & extent of muscle contraction to ensure smooth, accurate, & coordinated movements.
- Cerebellum sends its “blueprint” for coordinating movement to the cerebral motor cortex via the superior peduncles. It also sends info to brainstem nuclei → influences motor neurons of the spinal cord.
- Analogy
- Just as an ‘autopilot’ compares a plane’s instruments with its planned course, the cerebellum continually compares the higher brain’s intention with the body’s performance & makes appropriate corrections.

Descending tracts involved in motor functions
Descending motor pathways
Lateral pathways
- Roles
- Both tracts – voluntary movement of distal extremities
- Particularly hands & feet
- 2 divisions
- Corticospinal tract
- Originates in primary motor cortex
- Run through the internal capsule to the brainstem
- Decussate in medullary pyramids (medulla)
- Rubrospinal tract
- Originates in red nucleus of midbrain
- Decussate immediately below red nucleus (in the pons) → →
- Continue down the spinal cord in the lateral white matter
- Terminate in ventral horn of spinal grey matter
- Corticospinal tract
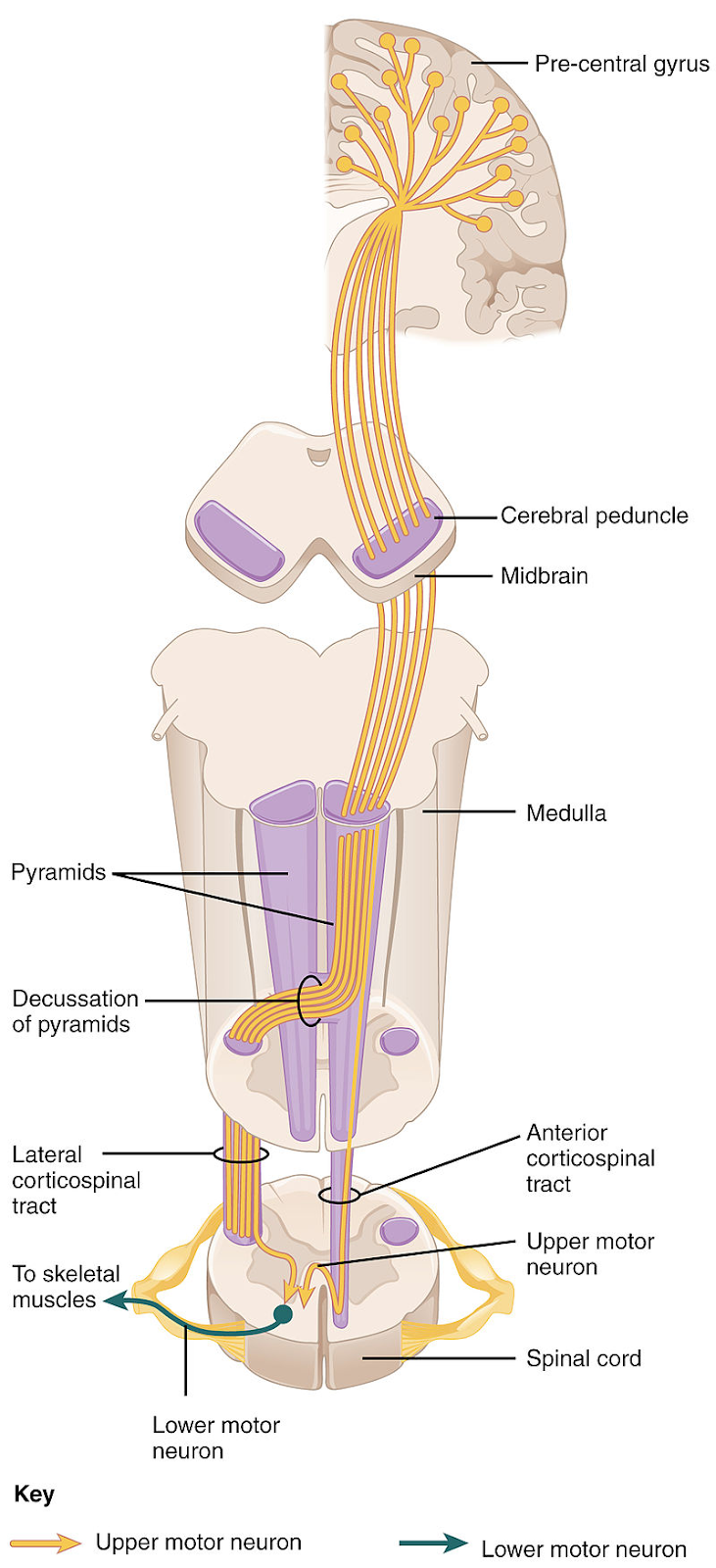
Ventromedial (indirect/extrapyramidal pathways)
Tectospinal (aka “colliculospinal”) tract
- Begins in the superior colliculus
- Decussates between midbrain & pons
- Function → visual tracking (head/eye coordination)
Vestibulospinal tract
- Begins in the vestibular nuclei of the medulla
- Does not decussate
- Function → maintain balance during standing & moving
Pontine & medullary reticulospinal tracts
- Begin in the pontine reticular formation
- Do not decussate
- Function → maintains muscle tone & visceral motor functions



- Note: These descending ‘upper motor neurons’ terminate in the ventral grey horns of the spinal cord grey matter by synapsing with either:
- Spinal interneurons – enabling info to be sent to multiple outputs
- Some interneurons are “central pattern generators”→ generate timing for patterned movements (e.g., walking)
- Or lower motor neurons – that directly innervate skeletal muscle
- Spinal interneurons – enabling info to be sent to multiple outputs
Somatic reflexes
- Rapid, automatic responses to stimuli
- Occur over neutral pathways called reflex arcs
- Components of a reflex arc
- Receptor → sensory neuron → CNS integration center → motor neuron → effector

Visceral reflexes
- Similar to somatic-NS, the ANS also has reflex arcs
- Visceral reflex arcs components
- Visceral sensory neurons (chemical changes/stretch/irritation of viscera) → ganglionic neuron (integration center) → motor neuron → effector


The Autonomic Nervous System
Divisions of the autonomic nervous system
The 2 divisions of the ANS (sympathetic & parasympathetic) serve the same visceral organs, but cause opposite effects. This dual innervation counterbalances each division’s activities → maintains homeostasis.
Sympathetic
- “Fight/flight”
- Mobilizes the body during activity
- Effects are widespread
Parasympathetic
- “Rest/digest”
- Conserves body energy & promotes maintenance functions
- Has relatively short-lived effects (due to short-acting nature of ACh)
- Effects are relatively localized


Efferent pathways and ganglia
As opposed to the somatic-NS which uses a mono-synaptic system (& hence lacks ganglia), the autonomic-NSuses a 2-neuron-chain system.
Preganglionic neuron
- The cell-body of the first neuron
- Resides in the brain or spinal cord
- Synapses with a ganglionic neuron
Ganglionic neuron
- Resides in an ‘autonomic ganglion’ outside the CNS
- Extends from the ganglion to the effector organ
Sympathetic & parasympathetic divisions differ anatomically in 3 ways
- Site of origin
- Fiber lengths
- Location of ganglia
| Characteristic | Parasympathetic | Sympathetic |
| Origin | Craniosacral outflow: brainstem nuclei of CN III, VII, IX, X; spinal cord segments S2–S4 | Thoracolumbar outflow: lateral horn of gray matter of spinal cord segments T1–L2 |
| Location of ganglia | Ganglia in (intramural) or close to visceral organ served | Ganglia within a few cm of CNS: alongside vertebral column (sympathetic trunk, or chain, ganglia) and anterior to vertebral column (collateral, or prevertebral, ganglia) |
| Relative length of pre- and postganglionic fibers | Long preganglionic; short postganglionic | Short preganglionic; long postganglionic |

Anatomy: the parasympathetic (craniosacral) division
- Fibers originate from brainstem & sacral region of spinal cord
- Preganglionic fibers – extend nearly all the way to the structures to be innervated
- Postganglionic fibers – very short; extend from the terminal ganglia & synapse with effector cells
- Ganglia location: located very close to or within the target organs
The cranial outflow
- Fibers originate from cranial-nerve nuclei in the brainstem
- Fibers extend to their terminal ganglia via 4 of the paired CN
| CN III Oculomotor | Pupil constriction, lens accommodation (close sight) |
| CN VII Facial | Stimulate large glands in the head (nasal, lacrimal, submandibular, sublingual salivary) |
| CN IX Glossopharyngeal | Stimulate parotid salivary glands |
| CN X Vagus | Serves virtually all organs of the thoracic and abdominal cavities (except distal large intensities) |
The sacral outflow
- Fibers originate from neurons in the lateral gray matter of spinal cord segments S2–S4
- Fibers extend to their terminal ganglia via splanchnic nerves of the pelvic plexus
- Serve distal large intestine & the pelvic organs (bladder, ureters, reproductive organs)

Anatomy: the sympathetic (thoracolumbar) division
Note: Sympathetic-NS innervates more organs than the parasympathetic, and its effects are longer-lasting
Fiber origin
Cell bodies of preganglionic neurons in the lateral horns spinal cord segments T1→L2
Fiber lengths
- Preganglionic fibers
- Exit spinal cord via ventral root
- Pass through white ramus communicans
- Synapse adjoining sympathetic trunk (chain) ganglion)
- Note: Fibers are short
- Postganglionic fibers
- Exit sympathetic ganglion at/below/above their spinal level via grey ramus communicans
- Enters ventral spinal nerve at that level
- To the effector organs
Note: The color of the rami communicans reveals whether or not their fibers are
myelinated. (pre: myelinated, post: unmyelinated)
Ganglia location
- Sympathetic trunks (chains of ganglia) flank each side of the vertebral column from neck to pelvis
- Note: Although the sympathetic trunks exist along the length of the spinal cord, the fibers arise only from thoracic & lumbar cord segments

Physiology of the Autonomic Nervous System
Neurotransmitters of the PNS
- Afferent (sensory)
- Glutamate
- Calcitonin-gene-related peptide
- Substance P
- Efferent (motor)
- Somatic/voluntary (skeletal muscle)
- Acetylcholine (ACh)
- Autonomic
- Sympathetic
- Preganglionic → ACh (stimulate ganglia and adrenal medulla)
- Postganglionic → Norepinephrine (NE)
- Adrenal medulla → stimulated by ACh to release epinephrine and NE into blood
- Parasympathetic
- Preganglionic → ACh
- Postganglionic → ACh
- Sympathetic
- Somatic/voluntary (skeletal muscle)

- Somatic division
- Axons extend from CNS to effector (skeletal muscles)
- Typically thick, heavy myelinated
- High conduction speed
- Neurot is ACh, effect is always stimulatory
- Autonomic division
- Preganglionic axons extend from CNS and synapse with either:
- Peripheral autonomic ganglia OR
- Cells of the adrenal medulla
- Release ACh
- Postganglionic axons extend from ganglia to effectors and release either
- ACh → parasympathetic
- NE → sympathetic
- Adrenal medullary cells release NE and epinephrine into the blood
- Preganglionic axons extend from CNS and synapse with either:
Note: Preganglionic fibers are thin & lightly myelinated & postganglionic fibers are thinner & unmyelinated. Hence, conduction speed within the autonomic neurons is slow – much slower than somatic NS.
Receptors of the ANS
Parasympathetic (cholinergic (ACh) receptors)
Nicotinic
- Found on
- Motor end-plates of skeletal muscle → somatic
- Receptive regions of all ganglionic neurons (both sympathetic & parasympathetic)
- Hormone-producing cells of the adrenal medulla
- Action
- Binding of ACh → directly opens ion channels (:.ionotropic) → depolarize the postsynaptic cell → stimulatory
Muscarinic
- Found on
- All effector cells stimulated by postganglionic cholinergic fibers (i.e., All parasympathetic target organs & some sympathetic targets [eccrine sweat glands & some skeletal-muscle blood vessels])
- Action
- Binding of ACh → Activates the receptor’s G-protein, which detaches from the receptor → Causes an intra-cellular signaling cascade (:.metabotropic). → may be stimulatory or inhibitory depending on the subclass of muscarinic receptor on the target organ
- Tissue-specific receptor subtypes
- M1 – Brain
- M2 – Heart
- M3 – Smooth Muscle & Glands
Sympathetic (adrenergic receptors)
- Receptors that respond to NE/epinephrine
- May be excitatory or inhibitory depending on which subclass of receptor predominates in that organ. (Organs responsive to NE/Epi often have more than one receptor subclass)
- Alpha: α1/2
- Beta: β1/2/3

Clinical manipulation of the peripheral NS
Aim
Use NS to regulate organ function
Drugs
Mimic/enhance/block messages sent along the nerves
Problem
- Side effects – because the PNS only uses 2 neurotransmitters, side effects can be widespread
- E.g., some illicit drugs have sympathomimetic side effects
- Cocaine & amphetamines ↑↑ cardiovascular stimulation (tachycardia & hypertension)
- Can reduce side effects by
- Topical application
- Targeting the specific receptor subtypes with more specific drugs
- Targeting tissue-specific differences in receptor subtypes
Examples
Somatic NS
- ACh inhibitors: ↓Deactivation of ACh in synapse → ↑ACh action)
- Neuromuscular blockers (e.g., nicotinic antagonists)
Autonomic NS
- Sympathetic
- Agents that affect release/reuptake of catecholamines (NE, epi, & dopamine)
- Adrenergic agonists & antagonists
- Parasympathetic
- ACh inhibitors: ↓Deactivation of ACh in synapse→ ↑ACh action
- Muscarinic agonists & antagonists
Ganglionic blockers
- Drugs which block chemical transmission at autonomic ganglia – essentially denervates the entire autonomic nervous system (main effect – vasodilation [loss of vasomotor tone])
- Effects vary from tissue to tissue, depending on whether sympathetic/parasympathetic nerves are usually dominant in that tissue:
- If sympathetic usually dominates, ganglionic blockers mimic parasympathetic stimulation
- If parasympathetic usually dominates, ganglionic blockers mimic sympathetic stimulation




Sympathetic and parasympathetic tone
Sympathetic (vasomotor) tone
- The continual state of partial constriction of the vascular system that maintains BP (even @ rest)
- During activity, a higher BP is needed → the vasomotor fibers fire more rapidly → vasoconstriction
- Note: Alpha-blockers dull the effects of the sympathetic/vasomotor tone → control hypertension
Parasympathetic tone
- Slows the heart, sets the normal activity levels of the digestive & urinary systems, & stimulates glandular secretion (except adrenal glands & skin glands)
- Note: The sympathetic division overrides this during times of stress
- Note: Drugs that block parasympathetic responses → ↑hr, fecal/urinary retention & ↓glandular secretion
Unique roles of the sympathetic NS
- Note: The sympathetic division is more wide-spread than the parasympathetic division – because it innervates more organs.
- E.g., adrenal medulla, sweat glands, hair-follicle muscles of the skin, the kidneys, & most blood vessels only receive sympathetic fibers
- There are other uniquely sympathetic functions
- Thermoregulatory response to heat
- Cutaneous vasodilation
- Activation of sweat glands
- Thermoregulatory response to cold
- Cutaneous vasoconstriction
- Release of renin from the kidneys
- Sympathetic impulses stimulate renin release
- Promotes increased BP
- Metabolic effects
- Sympathetic stimulation → of of adrenal medullary hormones
- Increased metabolic rate of body cells
- Increased blood glucose
- Mobilizes fat for use as fuels
- Puts skeletal muscle on red alert (contract more strongly and quickly)
- Sympathetic stimulation → of of adrenal medullary hormones
- Thermoregulatory response to heat
Central control of the autonomic NS
- ANS activity is regulated by a hierarchy of CNS controls
- Hypothalamus
- Brainstem
- Spinal cord
- Note: Subconscious cerebral inputs via limbic lobe influences hypothalamic functioning
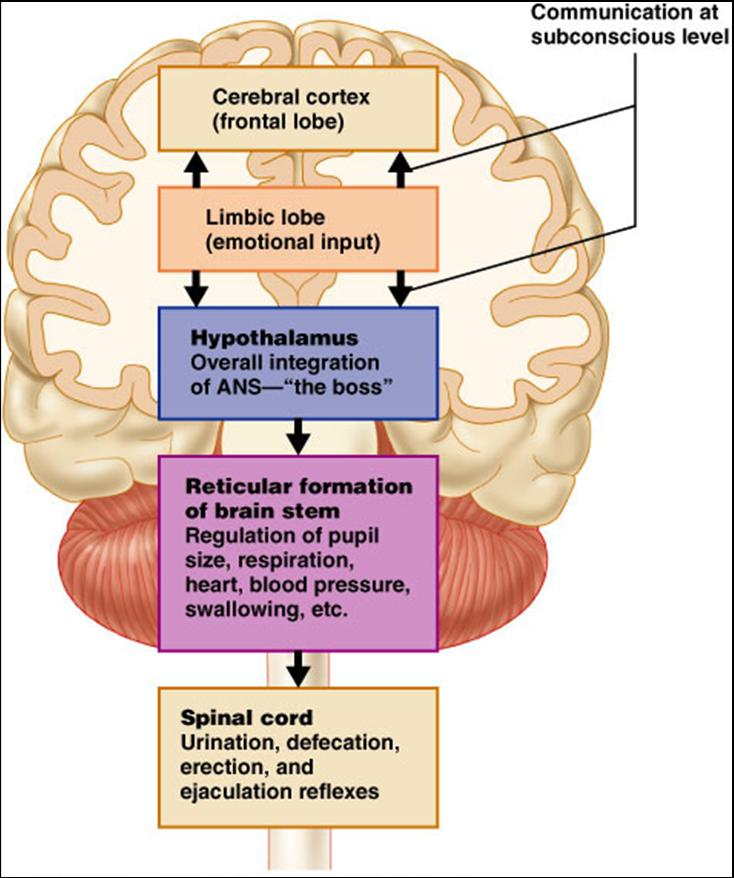
Disorders of the peripheral nervous system
Categories
- Inflammation
- Guillain Barre syndrome – immune mediated demyelinating neuropathy
- Myasthenia gravis – antibody attack on nicotinic ACh receptor in NMJ
- Trauma
- Spinal injuries
- Metabolic
- Diabetic neuropathies – macro/micro-vascular
- Vitamin deficiencies (B12, B6, E)
- Toxicity
- Urea
- Alcohol
- Genetics
- Infection
- Shingles
- Diphtheria
- Leprosy
Examples of homeostatic imbalances of the ANS
Hypertension
- Results from overactive sympathetic vasoconstriction promoted by chronic stress
- Can be treated with β-blockers, other adrenergic antagonists
Raynaud’s disease
- Characterized by intermittent attacks of peripheral cyanosis
- Provoked by exposure to cold or emotional stress
- An exaggerated vasoconstriction response
Autonomic dysreflexia
- Uncontrolled activation of autonomic neurons (mechanism unclear) in patients with quadriplegia
- Increased arterial BP, headache, flushed face, sweating
- Life-threatening