Cholelithiasis and Cholecystitis
Cholelithiasis is the formation of gallstones, which are hardened deposits of digestive fluids that are produced inside the gallbladder. Gallstones are made up of either cholesterol or pigment stones. Gallstones are not necessarily a serious problem; however it may lead to an obstruction in the normal flow of bile, causing cholecystitis. Cholecystitis is an inflammation of the gallbladder. The inflammation of the gallbladder occurs when the bile gets trapped inside the gallbladder as the gallstones block the bile from leaving the organ. This causes an infection with bacteria. There are two types of cholecystitis. Acute cholecystitis could be calculous or acalculous. On the other hand, chronic cholecystitis is associated with gallstone formation and it could follow acute cholecystitis; however, it occurs independently.
Nursing Diagnoses
Fluid volume, risk for deficient
Risk factors may include
- Excessive losses through gastric suction; vomiting, distension, and gastric hypermotility
- Medically restricted intake
- Altered clotting process
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired outcomes
- Demonstrate adequate fluid balance evidenced by stable vital signs, moist mucous membranes, good skin turgor, capillary refill, individually appropriate urinary output, absence of vomiting.
Nursing interventions
| INTERVENTION | RATIONALE |
| Maintain accurate record of I&O, noting output less than intake, increased urine specific gravity. Assess skin and mucous membranes, peripheral pulses, and capillary refill. | To provide information about fluid status and circulating volume needing replacement. |
| Monitor for signs and symptoms of increased or continued nausea or vomiting, abdominal cramps, weakness, twitching, seizures, irregular heart rate, paresthesia, hypoactive or absent bowel sounds, depressed respirations. | Prolonged vomiting, gastric aspiration, and restricted oral intake can lead to deficits in sodium, potassium, and chloride. |
| Eliminate noxious sights or smells from the environment. | Reduces stimulation of the vomiting center. |
| Perform frequent oral hygiene with alcohol-free mouthwash; apply lubricants. | Decreases dryness of oral mucous membranes; reduces risk of oral bleeding. |
| Use small-gauge needles for injections and apply firm pressure for longer than usual after venipuncture. | Reduces trauma, risk of bleeding or hematoma formation. |
| Assess for unusual bleeding: oozing from injection sites, epistaxis, bleeding gums, ecchymosis, petechiae, hematemesis or melena. | Prothrombin is reduced and coagulation time prolonged when bile flow is obstructed, increasing risk of bleeding or hemorrhage. |
| Keep patient NPO as necessary. | Decreases GI secretions and motility. |
| Insert NG tube, connect to suction, and maintain patency as indicated. | To rest the GI Tract |
Acute pain
- Biological injuring agents: obstruction/ductal spasm, inflammatory process, tissue ischemia/necrosis
Possibly evidenced by
- Reports of pain, biliary colic (waves of pain)
- Facial mask of pain; guarding behavior
- Autonomic responses (changes in BP, pulse)
- Self-focusing; narrowed focus
Desired outcomes
- Report pain is relieved/controlled.
- Demonstrate use of relaxation skills and diversional activities as indicated for individual situations.
Nursing interventions
| INTERVENTION | RATIONALE |
| Observe and document location, severity (0–10 scale), and character of pain (steady, intermittent, colicky). | Assists in differentiating cause of pain, and provides information about disease progression and resolution, development of complications, and effectiveness of interventions. |
| Note response to medication, and report to physician if pain is not being relieved. | Severe pain not relieved by routine measures may indicate developing complications or need for further intervention. |
| Promote bedrest, allowing the patient to assume a position of comfort. | Bedrest in low-Fowler’s position reduces intra-abdominal pressure; however, the patient will naturally assume the least painful position. |
| Use soft or cotton linens; calamine lotion, oil bath; cool or moist compresses as indicated. | Reduces irritation and dryness of the skin and itching sensation. |
| Control environmental temperature. | Cool surroundings aid in minimizing dermal discomfort. |
| Encourage use of relaxation techniques. Provide diversional activities. | Promotes rest, redirects attention, and may enhance coping. |
| Make time to listen to and maintain frequent contact with the patient. | Helpful in alleviating anxiety and refocusing attention, which can relieve pain. |
| Maintain NPO status, insert and/or maintain NG suction as indicated. | Removes gastric secretions that stimulate release of cholecystokinin and gallbladder contractions. |
Administer medications as indicated
| INTERVENTION | RATIONALE |
| Anticholinergics: atropine, propantheline (Pro-Banthı-ne) | Relieves reflex spasm and smooth muscle contraction and assists with pain management. |
| Sedatives: phenobarbital | Promotes rest and relaxes smooth muscle, relieving pain. |
| Narcotics: meperidine hydrochloride (Demerol), morphine sulfate | Given to reduce severe pain. Morphine is used with caution because it may increase spasms of the sphincter of Oddi, although nitroglycerin may be given to reduce morphine-induced spasms if they occur. |
| Monoctanoin (Moctanin) | This medication may be used after a cholecystectomy for retained stones or for newly formed large stones in the bile duct. It is a lengthy treatment (1–3 wk) and is administered via a nasal-biliary tube. A cholangiogram is done periodically to monitor stone dissolution. |
| Smooth muscle relaxants: papaverine (Pavabid), nitroglycerin, amyl nitrite | Relieves ductal spasm |
| Chenodeoxycholic acid (Chenix), ursodeoxycholic acid (Urso, Actigall) | These natural bile acids decrease cholesterol synthesis, dissolving gallstones. Success of this treatment depends on the number and size of gallstones (preferably three or fewer stones smaller than 20 min in diameter) floating in a functioning gallbladder. |
| Antibiotics | To treat infectious processes, reducing inflammation. |
Nutrition: Less than body requirements, risk for imbalance
Risk factors may include
- Self-imposed or prescribed dietary restrictions, nausea/vomiting, dyspepsia, pain
- Loss of nutrients; impaired fat digestion due to obstruction of bile flow
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired outcomes
- Report relief of nausea/vomiting.
- Demonstrate progression toward desired weight gain or maintain weight as individually appropriate.
Nursing interventions
| INTERVENTION | RATIONALE |
| Calculate caloric intake. Keep comments about appetite to a minimum. | Identifies nutritional deficiencies and/or needs. Focusing on the problem creates a negative atmosphere and may interfere with intake. |
| Weigh as indicated. | Monitors effectiveness of dietary plan. |
| Consult with the patient about likes and dislikes, foods that cause distress, and preferred meal schedule. | Involving the patient in planning enables the patient to have a sense of control and encourages eating. |
| Provide a pleasant atmosphere at mealtime; remove noxious stimuli. | Useful in promoting appetite/reducing nausea. |
| Provide oral hygiene before meals. | A clean mouth enhances appetite. |
| Offer effervescent drinks with meals, if tolerated. | May lessen nausea and relieve gas. Note:May be contraindicated if the beverage causes gas formation/gastric discomfort. |
| Assess for abdominal distension, frequent belching, guarding, reluctance to move. | Nonverbal signs of discomfort associated with impaired digestion, gas pain. |
| Ambulate and increase activity as tolerated. | Helpful in expulsion of flatus, reduction of abdominal distension. Contributes to overall recovery and sense of well-being and decreases possibility of secondary problems related to immobility (pneumonia, thrombophlebitis). |
| Consult with a dietitian or nutritional support team as indicated. | Useful in establishing individual nutritional needs and the most appropriate route. |
| Begin a low-fat liquid diet after the NG tube is removed. | Limiting fat content reduces stimulation of gallbladder and pain associated with incomplete fat digestion and is helpful in preventing recurrence. |
| Advance diet as tolerated, usually low-fat, high-fiber. Restrict gas-producing foods (onions, cabbage, popcorn) and foods or fluids high in fats (butter, fried foods, nuts). | Meets nutritional requirements while minimizing stimulation of the gallbladder. |
| Administer bile salts: Bilron, Zanchol, dehydrocholic acid (Decholin), as indicated. | Promotes digestion and absorption of fats, fat-soluble vitamins, cholesterol. Useful in chronic cholecystitis. |
| Monitor laboratory studies: BUN, prealbumin, albumin, total protein, transferrin levels. | Provides information about nutritional deficits or effectiveness of therapy. |
| Provide parenteral and/or enteral feedings as needed. | Alternative feeding may be required depending on degree of disability and gallbladder involvement and need for prolonged gastric rest. |
Deficient knowledge
- Lack of knowledge/recall
- Information misinterpretation
- Unfamiliarity with information resources
Possibly evidenced by
- Questions; request for information
- Statement of misconception
- Inaccurate follow-through of instruction
- Development of preventable complications
Desired outcomes
- Verbalize understanding of disease process, prognosis, potential complications.
- Verbalize understanding of therapeutic needs.
- Initiate necessary lifestyle changes and participate in treatment regimen.
Nursing interventions
| INTERVENTION | RATIONALE |
| Explain reasons for test procedures and preparations as needed. | Information can decrease anxiety, thereby reducing sympathetic stimulation. |
| Review disease process and prognosis. Discuss hospitalization and prospective treatment as indicated. Encourage questions, expression of concern. | Provides a knowledge base from which the patient can make informed choices. Effective communication and support at this time can diminish anxiety and promote healing. |
| Review drug regimen, possible side effects. | Gallstones often recur, necessitating long-term therapy. Development of diarrhea or cramps during chenodiol therapy may be dose-related or correctable. Note: Women of childbearing age should be counseled regarding birth control to prevent pregnancy and risk of fetal hepatic damage. |
| Discuss weight reduction programs if indicated | Obesity is a risk factor associated with cholecystitis, and weight loss is beneficial in medical management of chronic conditions. |
| Instruct the patient to avoid food/fluids high in fats (pork, gravies, nuts, fried foods, butter, whole milk, ice cream), gas producers (cabbage, beans, onions, carbonated beverages), or gastric irritants ( spicy foods, caffeine, citrus). | Limits or prevents recurrence of gallbladder attacks. |
| Review signs and symptoms requiring medical intervention: recurrent fever; persistent nausea and vomiting, or pain; jaundice of skin or eyes, itching; dark urine; clay-colored stools; blood in urine, stools, vomitus; or bleeding from mucous membranes. | Indicative of progression of disease process and development of complications requiring further intervention. |
| Recommend resting in a semi-Fowler’s position after meals. | Promotes flow of bile and general relaxation during the initial digestive process. |
| Suggest the patient to limit gum chewing, sucking on straw and hard candy, or smoking. | Promotes gas formation, which can increase gastric distension and discomfort. |
| Discuss avoidance of aspirin-containing products, forceful blowing of nose, straining for bowel movement, contact sports. | Reduces risk of bleeding related to changes in coagulation time, mucosal irritation, and trauma. |
| Recommend use of soft toothbrush, electric razor. | Reduces risk of bleeding related to changes in coagulation time, mucosal irritation, and trauma. |
Nursing Notes
Risk factors
| Cholelithiasis | Cholelithiasis |
| Results from changes in bile components or bile stasis, associated with:InfectionCirrhosisPancreatitisCeliac diseaseDiabetes mellitusPregnancyHormonal contraceptive use | Obstruction of the cystic duct by an impacted gallstoneTissue damage due to trauma, massive burns, or surgeryGram-negative septicemiaMultiple blood transfusionProlonged fastingHypertensionOveruse of opioid analgesics |
Pathophysiology
Cholelithiasis
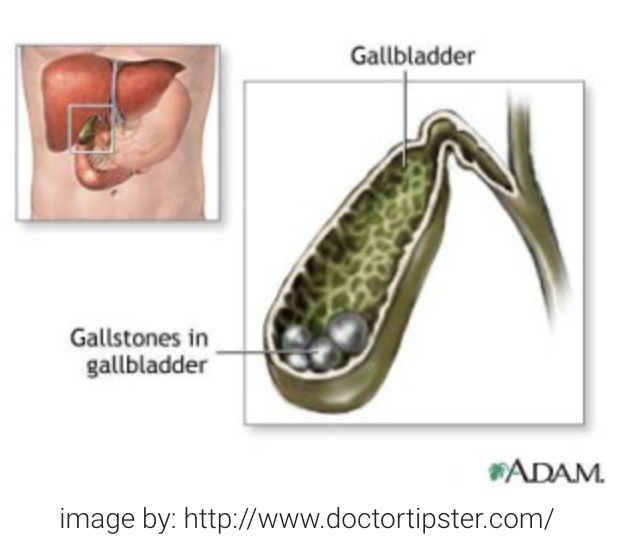
Calculi usually from solid constituents of bile; the three major types are:
- Cholesterol gallstones – the most common type, thought to form in supersaturated bile
- Pigment gallstones – formed mainly of unconjugated pigments in bile precipitate
- Mixed types – with characteristics of pigment and cholesterol stones.
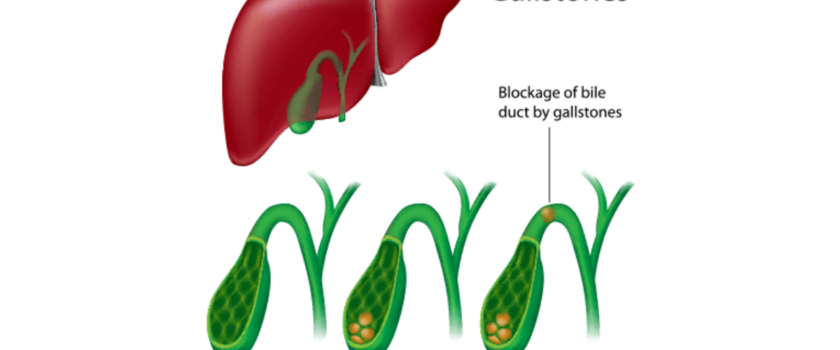
Gallstones can obstruct the cystic duct, causing cholecystitis, or the common bile duct, which is called choledocholithiasis.
Cholecystitis
- In acute and chronic cholecystitis, inflammation causes the gallbladder wall to become thickened and edematous and causes the cystic lumen to increase in diameter.
- If inflammation spreads to the common bile duct, obstruction of bile drainage can lead to jaundice. Other possible complications include: (Empyema i.e. pus-filled gallbladder, perforation, emphysematous cholecystitis)
Assessment/clinical manifestations/signs and symptoms
Cholelithiasis (up to ½ of persons with gallstones are asymptomatic; however possible clinical manifestations include the following)
- Episodic (commonly after a high-fat meal), cramping pain in the right upper abdominal quadrant or the epigastrium, possibly radiating to the back near the right scapular tip (i.e. biliary colic)
- Nausea and vomiting
- Fat intolerance
- Fever and leukocytosis
- Signs and symptoms of jaundice
| Acute Cholecystitis | Chronic Cholecystitis |
| Biliary colicTenderness and rigidity in the right upper quadrant elicited on palpation (i.e. Murphy’s sign)FeverNausea and vomitingFat intoleranceSigns and symptoms of jaundice | Pain, which is less severe than in the acute formFever, which is less severe than in the acute formFat intoleranceHeartburnFlatulence |
Laboratory and Diagnostic Study Findings
Cholelithiasis
- Biliary ultrasonography (i.e. cholecystosonography) can detect gallstones in most cases.
Cholecystitis
- White blood cell count reveals leukocytosis
- Serum alkaline phosphatase is elevated
- Ultrasonography detects gallstone
- Endoscopic retrograde cholangiopancreatography may reveal inflamed common bile ducts, gallbladder, and gallstones.
- Percutaneous transhepatic cholangiography can identify gallstones within the bile ducts.
Medical management
Teach the client about planned treatments.
- Chenodeoxycholic acid is administered to dissolve gallstones. It is effective in dissolving about 60% of radiolucent gallstones. Pigment gallstones cannot be dissolved and must be excised.
- Nonsurgical removal, such as lithotripsy or extracorporeal shock wave therapy, may be implemented.
Surgical treatment may be ordered.
Laparoscopic cholecytectomy (usually outpatient surgery) is performed through a small incision made through the abdominal wall in the umbilicus.
- Assess incision sites for infection. Instruct the client to notify the health care provider if loss of appetite, vomiting, pain, abdominal distention, or fever occur.
- Advise the client that he will need assistance at home for 2 to 3 days.
Cholecystectomy is removal of the gallbladder after ligation of the cystic duct and artery. Inform the client that a T-tube will be inserted to drain blood; serosanguineous fluids, and bile and that the T-tube must be taped below the incision
Choledochostomy is an incision into the common bile duct for calculi removal.
Cholecystomy is the surgical opening of the gallbladder for removal of stones, bile, or pus, after which a drainage tube is placed.
Nursing diagnosis
- Acute pain secondary to biliary obstruction
- Ineffective coping related to nausea
- Deficient knowledge related to diagnosis
- Impaired gas exchange related to high abdominal surgical incision.
- Impaired skin integrity related to altered biliary drainage after surgical incision.
- Imbalanced nutrition related to inadequate bile secretion.
Nursing management
Provide nursing interventions during an acute gallbladder attack.
- Intervene to relieve pain; give prescribed analgesics
- Promote adequate rest
- Administer IV fluids, monitor intake and output
- Monitor nasogastric tube and suctioning
- Administer antibiotics if prescribed.
Provide adequate nutrition.
- Assess nutritional status. Encourage a high-protein, high-carbohydrate, low-fat diet.